Full Code CPR: Complete Guide to General CPR Knowledge in 2026 July
🧠 Master full code CPR with our complete guide covering ACLS algorithm, infant CPR, AED usage, BLS certification, and life support fundamentals for 2026 July.
Understanding full code CPR is the foundation of emergency medical response, encompassing every life-saving intervention from chest compressions to advanced cardiac life support. When a patient is designated full code, it means medical providers will perform all necessary measures to revive them during cardiac or respiratory arrest, including CPR, defibrillation, intubation, and pharmacological intervention. This comprehensive guide explores general CPR knowledge that every responder, from lay rescuer to healthcare professional, must master to effectively respond to sudden cardiac emergencies in any setting.
The acls algorithm sits at the heart of advanced resuscitation, providing a systematic decision-tree that healthcare providers follow during cardiac arrest events. It integrates rhythm recognition, drug administration timing, and electrical therapy into a cohesive sequence that maximizes the chance of return of spontaneous circulation. Mastering this algorithm requires understanding not just the steps, but the reasoning behind each intervention and how they interconnect with basic CPR techniques performed simultaneously by the resuscitation team.
According to the American Heart Association's 2025 guidelines, over 350,000 out-of-hospital cardiac arrests occur annually in the United States, with survival rates hovering around 10% when bystander CPR is not initiated. However, when high-quality CPR begins within the first minute, survival rates can triple or even quadruple. These statistics underscore why widespread CPR training matters, and why organizations like the national cpr foundation continue expanding accessible certification programs across communities, schools, and workplaces nationwide.
Whether you're preparing for your first basic life support course or refreshing skills as an experienced clinician, this guide consolidates the most current evidence-based practices. We'll cover everything from compression depth and rate to AED operation, infant resuscitation modifications, recovery positioning, and the differences between BLS, ACLS, and PALS certifications. You can also explore our cpr cell phone repair resource for deeper certification preparation materials.
One of the most important conceptual shifts in modern CPR education is the emphasis on hands-only chest compressions for untrained bystanders. Research published in the New England Journal of Medicine demonstrated that compression-only CPR produces survival outcomes comparable to traditional CPR with rescue breaths for adult sudden cardiac arrest victims. This simplification removes a major barrier to bystander action, particularly concerns about mouth-to-mouth contact with strangers during a crisis.
However, full conventional CPR with rescue breaths remains the gold standard for pediatric victims, drowning cases, and prolonged arrests where oxygen reserves have been depleted. Understanding when to apply each technique requires both formal training and ongoing practice. This article will help you build that judgment by walking through scenarios, decision frameworks, and the specific protocols that govern different patient populations and emergency contexts.
By the end of this comprehensive guide, you'll have a solid grasp of general CPR knowledge that prepares you for certification exams, workplace requirements, and real-world emergencies. We've structured each section to build progressively, starting with fundamentals and advancing to specialized topics like advanced airway management, post-resuscitation care, and team dynamics during a code blue event in clinical settings.
Full Code CPR by the Numbers
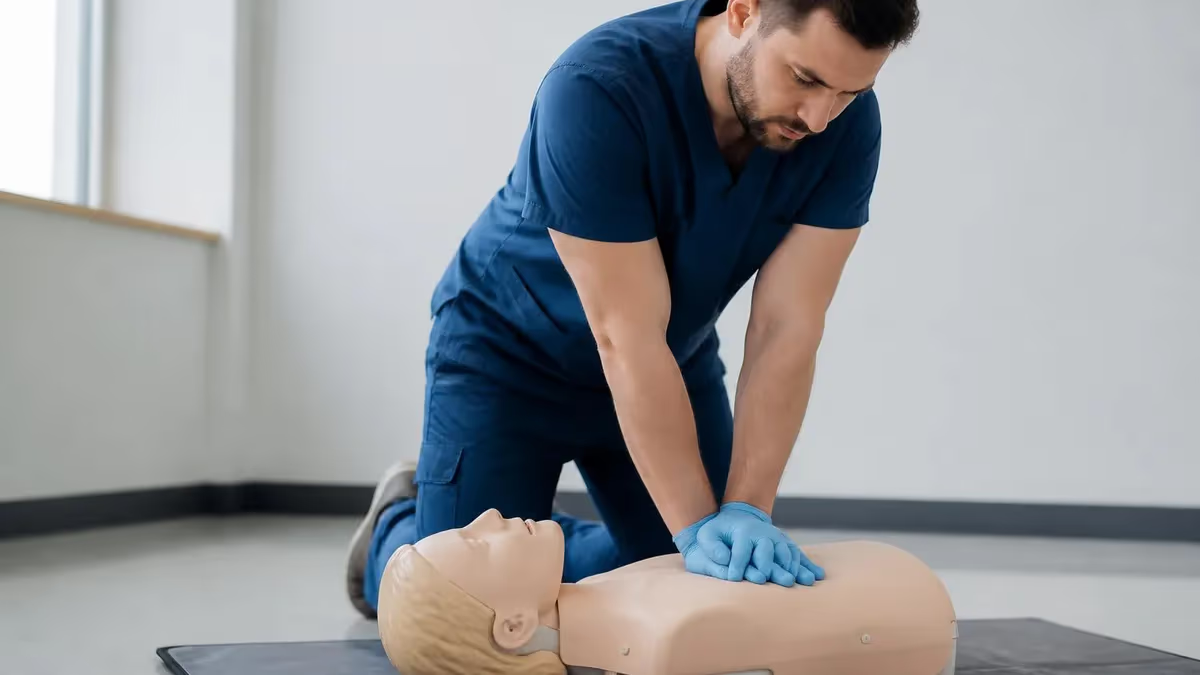
Core Steps of Full Code CPR
Before approaching any victim, ensure the scene is safe from traffic, electrical hazards, fire, or violence. Don personal protective equipment if available, and quickly evaluate the situation to avoid becoming a second victim during your rescue attempt.
Tap the victim's shoulders firmly and shout 'Are you okay?' Look for normal breathing for no more than 10 seconds. Agonal gasps are not normal breathing and indicate cardiac arrest requiring immediate compressions.
Call 911 immediately or direct a bystander to do so. Request an AED if available. In hospital settings, call a code blue. Put your phone on speaker so you can communicate while beginning compressions without delay.
Place the heel of your hand on the lower half of the sternum, interlock fingers, and push hard and fast at 100-120 compressions per minute. Allow full chest recoil between compressions to maximize cardiac filling.
As soon as the AED arrives, power it on and follow voice prompts. If trained in rescue breathing, deliver 2 breaths after every 30 compressions, each lasting about 1 second and producing visible chest rise.
The acls algorithm provides a structured framework for managing cardiac arrest and peri-arrest situations in clinical settings. It begins with the BLS survey, transitions to the ACLS primary assessment, and branches based on the patient's cardiac rhythm. Shockable rhythms like ventricular fibrillation and pulseless ventricular tachycardia receive immediate defibrillation, while non-shockable rhythms like asystole and pulseless electrical activity rely on high-quality CPR, epinephrine, and aggressive search for reversible causes known as the H's and T's.
Epinephrine administration timing has been refined in recent guideline updates. For non-shockable rhythms, providers should administer 1 mg of epinephrine IV or IO as soon as feasible, then repeat every 3-5 minutes. For shockable rhythms, epinephrine is given after the second defibrillation attempt. This sequencing reflects evidence that early epinephrine in non-shockable rhythms improves return of spontaneous circulation, while delayed administration in shockable rhythms allows defibrillation to remain the primary intervention.
Quality metrics during ACLS are non-negotiable. Chest compression fraction—the percentage of arrest time during which compressions are actively performed—should exceed 80%. Compressions must be at the correct depth and rate, with full recoil between compressions. Modern defibrillators provide real-time feedback on these metrics, allowing the team leader to coach compressors and rotate them every two minutes to prevent fatigue-related quality decline.
The H's and T's represent reversible causes that must be identified and addressed during resuscitation. The H's include hypovolemia, hypoxia, hydrogen ion (acidosis), hypo/hyperkalemia, and hypothermia. The T's include tension pneumothorax, tamponade (cardiac), toxins, thrombosis (pulmonary), and thrombosis (coronary). Each requires specific interventions ranging from fluid boluses and intubation to needle decompression, pericardiocentesis, and thrombolytic therapy depending on the underlying pathology.
Advanced airway management during ACLS has shifted toward supraglottic devices like the i-gel or King LT for most providers, reserving endotracheal intubation for situations where it can be performed without significant interruption of compressions. Once an advanced airway is in place, the compression-to-ventilation cycle changes to continuous compressions with one breath every 6 seconds, eliminating the need for pauses during the 30:2 cycle. Capnography becomes the gold standard for confirming airway placement and monitoring resuscitation quality.
Team dynamics distinguish effective codes from chaotic ones. Clear role assignment, closed-loop communication, mutual respect, and a designated team leader who maintains situational awareness without performing tasks directly all contribute to better outcomes. Many institutions now run simulation-based training programs where teams practice these dynamics under realistic stress conditions. You can learn more in our what is a bls certification guide for exam preparation strategies.
Post-resuscitation care begins the moment spontaneous circulation returns. Targeted temperature management between 32-36°C, optimization of blood pressure and oxygenation, glycemic control, and prompt cardiac catheterization for suspected ischemic causes all improve neurological outcomes. The ACLS algorithm doesn't end with ROSC; it transitions into a comprehensive post-arrest bundle that often determines whether the patient walks out of the hospital neurologically intact.
CPR Practice Test Questions
Prepare for the CPR Cardiopulmonary Resuscitation Practice exam with our free practice test modules. Each quiz covers key topics to help you pass on your first try.
CPR Basic CPR
CPR Exam Questions covering Basic CPR. Master CPR Test concepts for certification prep.
CPR and First Aid
Free CPR Practice Test featuring and First Aid. Improve your CPR Exam score with mock test prep.
CPR (Cardiopulmonary Resuscitation) Adult ...
CPR Mock Exam on (Cardiopulmonary Resuscitation) Adult CPR and AED Usage. CPR Study Guide questions to pass on your first try.
CPR (Cardiopulmonary Resuscitation) Airway...
CPR Test Prep for (Cardiopulmonary Resuscitation) Airway Obstruction and Choking. Practice CPR Quiz questions and boost your score.
CPR (Cardiopulmonary Resuscitation) Cardio...
CPR Questions and Answers on (Cardiopulmonary Resuscitation) Cardiopulmonary Emergency Recognition. Free CPR practice for exam readiness.
CPR (Cardiopulmonary Resuscitation) Child ...
CPR Mock Test covering (Cardiopulmonary Resuscitation) Child and Infant CPR. Online CPR Test practice with instant feedback.
CPR (Cardiopulmonary Resuscitation) High-P...
Free CPR Quiz on (Cardiopulmonary Resuscitation) High-Performance Team Dynamics. CPR Exam prep questions with detailed explanations.
CPR (Cardiopulmonary Resuscitation) Legal ...
CPR Practice Questions for (Cardiopulmonary Resuscitation) Legal and Ethical Considerations. Build confidence for your CPR certification exam.
CPR for Specific Populations
CPR Test Online for for Specific Populations. Free practice with instant results and feedback.
CPR Airway & Breathing Management
CPR Exam Questions covering Airway & Breathing Management. Master CPR Test concepts for certification prep.
CPR Assessment & Recognition of Cardiac Ar...
Free CPR Practice Test featuring Assessment & Recognition of Cardiac Arrest. Improve your CPR Exam score with mock test prep.
CPR Chest Compressions & Defibrillation
CPR Mock Exam on Chest Compressions & Defibrillation. CPR Study Guide questions to pass on your first try.
CPR Post-Resuscitation Care & Recovery
CPR Test Prep for Post-Resuscitation Care & Recovery. Practice CPR Quiz questions and boost your score.
Infant CPR, Child CPR, and Adult Resuscitation
Infant cpr applies to babies under one year of age and uses two fingers placed just below the nipple line for compressions on the lower half of the sternum. Compression depth is approximately 1.5 inches or one-third the depth of the chest. The rate remains 100-120 per minute, and the compression-to-ventilation ratio is 30:2 for a single rescuer or 15:2 for two rescuers, reflecting infants' greater dependence on adequate oxygenation.
Rescue breaths for infants are delivered by covering both the nose and mouth with your mouth, providing just enough volume to make the chest rise visibly. Over-ventilation can cause gastric distention and impair circulation. Common causes of infant cardiac arrest are respiratory in origin, including SIDS, choking, and respiratory infections, which is why ventilation is emphasized more heavily than in adult resuscitation protocols.
Hands-Only CPR vs Conventional CPR: Which Is Better?
- +Easier for untrained bystanders to remember and execute under stress
- +No mouth-to-mouth concerns eliminate hesitation barriers
- +Equally effective for adult sudden cardiac arrest in first few minutes
- +Allows continuous chest compression without pauses for breaths
- +Dispatcher-assisted CPR instructions are simpler and faster
- +Increases bystander CPR rates significantly in community studies
- −Not appropriate for pediatric arrests or drowning victims
- −Less effective for prolonged arrests beyond 6-8 minutes
- −Doesn't replenish oxygen in respiratory-cause arrests
- −Inadequate for asphyxial arrest patterns common in children
- −Not the standard of care for trained healthcare providers
- −May produce worse outcomes in hypoxic arrest scenarios
Full Code CPR Performance Checklist
- ✓Ensure scene safety before approaching the victim and don PPE
- ✓Check responsiveness by tapping shoulders and shouting
- ✓Look for normal breathing for no more than 10 seconds
- ✓Call 911 or activate emergency response system immediately
- ✓Request an AED and direct bystanders to specific tasks
- ✓Begin chest compressions at 100-120 per minute with proper depth
- ✓Allow full chest recoil between each compression cycle
- ✓Switch compressors every 2 minutes to prevent fatigue
- ✓Attach AED as soon as available and follow voice prompts
- ✓Continue CPR until ALS arrives or victim shows signs of life
Brain Damage Begins Quickly Without CPR
Irreversible brain damage begins within 4-6 minutes of cardiac arrest without CPR. Every minute that passes without compressions and defibrillation decreases survival probability by approximately 7-10%. This is why bystander CPR initiated within the first minute of collapse can triple or even quadruple survival rates compared to waiting for EMS arrival.
The question 'what does aed stand for' comes up constantly in CPR courses, and the answer is automated external defibrillator. These portable devices analyze cardiac rhythms and deliver electrical shocks to restore normal heart function during sudden cardiac arrest. Modern AEDs are designed for use by laypeople with minimal training, providing voice prompts that guide users through pad placement, rhythm analysis, and shock delivery. They will only advise a shock when a shockable rhythm like ventricular fibrillation or pulseless ventricular tachycardia is detected.
Proper AED pad placement is critical for accurate rhythm analysis and effective shock delivery. The standard anterolateral placement positions one pad on the upper right chest below the clavicle and the other on the lower left side of the chest in the mid-axillary line. For patients with implanted pacemakers or defibrillators, place the pads at least one inch away from the device. If the chest is wet, dry it quickly before pad application. Excessive chest hair may require a second set of pads to be applied after removing the first to depilate the area.
Life support is a broad category encompassing basic life support, advanced cardiac life support, and pediatric advanced life support, each tailored to different patient populations and clinical scenarios. BLS focuses on high-quality CPR, AED use, and choking response—skills appropriate for all healthcare providers and lay rescuers. ACLS adds pharmacology, advanced airway management, and rhythm interpretation for adult patients. PALS extends these advanced concepts to pediatric populations with age-specific modifications.
Respiratory rate monitoring during and after resuscitation provides crucial information about the patient's oxygenation and ventilation status. Normal adult respiratory rate is 12-20 breaths per minute, while children breathe 20-30 times per minute, and infants 30-60 times per minute. During CPR with an advanced airway, providers deliver one breath every 6 seconds, equivalent to 10 breaths per minute. Avoiding hyperventilation is critical, as excessive ventilation increases intrathoracic pressure and reduces venous return to the heart.
Capnography has emerged as the most reliable indicator of CPR quality and return of spontaneous circulation. End-tidal CO2 values below 10 mmHg during CPR suggest inadequate compression quality or inability to achieve adequate perfusion, prompting compressor rotation or technique adjustment. A sudden rise in ETCO2 to 35-40 mmHg often signals return of spontaneous circulation before a palpable pulse can be confirmed, allowing the team to transition to post-arrest care without unnecessary continued compressions.
Recovery position should be used for unconscious patients who are breathing normally but cannot protect their airway. Roll the patient onto their side with the lower arm extended forward, upper leg bent at the knee for stability, and head tilted slightly back to maintain an open airway. This position prevents aspiration of vomit or secretions while you await EMS. Monitor breathing continuously and be ready to return the patient to their back if breathing stops or becomes irregular.
Modern resuscitation equipment has evolved significantly, with mechanical CPR devices like the LUCAS and AutoPulse providing consistent compression quality during transport and prolonged resuscitations. These devices don't replace human providers but supplement teams during transport, cath lab procedures, or extended resuscitations. Extracorporeal CPR, where venoarterial ECMO is initiated during ongoing resuscitation for refractory cardiac arrest, represents the cutting edge of resuscitation science in selected centers with rapid deployment protocols.
BLS, ACLS, and PALS certifications expire after exactly 2 years. Working with an expired certification can result in immediate loss of clinical privileges, employment termination, and licensure issues. Set calendar reminders 90 days before expiration to schedule renewal courses and avoid emergency credential gaps.
Understanding what is a bls certification helps you choose the right course for your needs. Basic Life Support certification is the foundational credential for healthcare providers, requiring demonstrated competency in adult, child, and infant CPR, AED operation, choking relief, and team-based resuscitation. The course typically takes 4-5 hours and is required for nurses, doctors, paramedics, dental staff, and most allied health professionals. The American Heart Association BLS course remains the most widely recognized certification, though the American Red Cross offers equivalent credentialing.
Pals certification, or Pediatric Advanced Life Support, builds on BLS skills with pediatric-specific assessment, pharmacology, and treatment algorithms for infants and children up to puberty. The 14-16 hour course covers the systematic pediatric assessment, recognition of shock and respiratory failure, rhythm disturbances unique to pediatric populations, and team dynamics in pediatric resuscitation. PALS is essential for emergency department staff, pediatric units, urgent care providers, and any clinician who may encounter pediatric emergencies in their practice.
ACLS certification represents the next tier of training for providers managing adult cardiovascular emergencies. The 14-16 hour course covers the acls algorithm in depth, including rhythm recognition, pharmacological interventions, advanced airway management, and post-arrest care. ACLS is required for ICU nurses, emergency physicians, anesthesiologists, and critical care providers. Some institutions also require ACLS for medical-surgical nurses and rapid response team members, reflecting the growing emphasis on early intervention before full cardiac arrest occurs.
The national cpr foundation is one of several organizations offering CPR certification courses, with online and blended learning options that appeal to busy professionals. When choosing a certification provider, verify that the credential is accepted by your employer or licensing body. AHA and Red Cross certifications are universally accepted in the United States, while some online-only providers may not satisfy employer requirements. Always confirm acceptability before enrolling in a course, especially for healthcare positions with strict credentialing standards.
Recertification typically requires demonstrating competency through skills checks and written examinations every two years. Many providers offer 'challenge' courses for experienced clinicians, allowing them to test out of didactic portions if they can demonstrate mastery during initial skills assessment. Online refresher courses combined with in-person skills verification have become increasingly common, offering flexibility while maintaining hands-on competency standards. Explore our cpr index for more on hybrid certification options.
Beyond formal certifications, many professionals pursue specialized training in areas like ECMO, mechanical circulatory support, and advanced resuscitation team leadership. These competencies often require institutional credentialing rather than national certifications, but they reflect the growing complexity of modern resuscitation practice. Simulation training has become a cornerstone of skill maintenance, with high-fidelity manikins and immersive scenarios providing safe environments to practice rare but critical interventions before encountering them with real patients.
Workplace CPR training is increasingly mandated for non-healthcare professionals as well. Teachers, lifeguards, fitness instructors, daycare workers, and security personnel often must maintain current CPR certification. Some states require CPR training as a high school graduation requirement, creating a generation of citizens prepared to respond to cardiac emergencies in their communities. This grassroots expansion of CPR competency represents one of the most important public health initiatives of the past two decades.
Practical preparation for CPR competency goes beyond memorizing protocols. Regular hands-on practice with manikins, ideally in scenarios that mimic real-world stress, builds the muscle memory and decision-making confidence needed during actual emergencies. Many providers find that monthly mock codes within their workplaces dramatically improve real performance compared to relying solely on biennial certification courses. The cognitive load during real arrests is enormous, and only practiced responses survive the stress response intact.
For lay rescuers, the most important preparation is overcoming the hesitation to act. Studies consistently show that fear of doing harm, fear of legal liability, and uncertainty about correct technique prevent bystanders from attempting CPR. Good Samaritan laws in all 50 states protect lay rescuers from liability when acting in good faith. The reality is that doing nothing guarantees death, while attempting CPR offers the only chance of survival. Even imperfect CPR is dramatically better than no CPR at all.
Equipment familiarity matters as much as technique. Walk through your workplace, gym, school, or community spaces and locate AEDs before you need them. Many facilities now register their AEDs with PulsePoint and similar apps that direct nearby trained responders to cardiac emergencies. Understanding where life-saving equipment lives in your daily environment converts theoretical knowledge into rapid action when seconds matter. Take a moment after reading this article to identify the nearest AED in your current location.
Maintaining physical fitness contributes to CPR effectiveness in ways many providers underestimate. High-quality chest compressions are physically demanding, and fatigue degrades quality after just 1-2 minutes. Healthcare workers who maintain reasonable cardiovascular and upper body fitness deliver better compressions for longer durations. This isn't about elite fitness but about basic physical capability to sustain effort during emergencies that often require multiple compressors and prolonged efforts.
Mental rehearsal techniques borrowed from athletes and military trainers help CPR providers prepare for the stress of real emergencies. Visualization of yourself successfully navigating a code blue, including the smells, sounds, and chaos of a real resuscitation, primes your nervous system to perform under pressure. Combined with regular skills practice, mental rehearsal can significantly reduce performance degradation during actual events when adrenaline and uncertainty would otherwise impair clear thinking.
Stay current with guideline updates by subscribing to AHA newsletters, attending professional conferences, or reading resuscitation journals. The science evolves continuously, with significant updates roughly every five years and minor updates between cycles. Practitioners who learned CPR in 2010 are practicing outdated protocols if they haven't recertified or refreshed their knowledge. The 2025 guidelines incorporated meaningful changes to compression depth recommendations, epinephrine timing, and post-arrest care that improve outcomes when properly applied.
Finally, build a peer support network for debrief after real resuscitation events. Whether the outcome is positive or negative, processing the experience with colleagues who understand the work prevents emotional accumulation that contributes to burnout and PTSD among healthcare providers. Many institutions now mandate post-event debriefing, but informal peer support remains equally valuable. Caring for yourself enables you to continue caring for others, sustaining a long career of life-saving practice.
CPR Questions and Answers




About the Author
Registered Nurse & Healthcare Educator
Johns Hopkins University School of NursingDr. Sarah Mitchell is a board-certified registered nurse with over 15 years of clinical and academic experience. She completed her PhD in Nursing Science at Johns Hopkins University and has taught NCLEX preparation and clinical skills courses for nursing students across the United States. Her research focuses on evidence-based exam preparation strategies for healthcare certification candidates.
Join the Discussion
Connect with other students preparing for this exam. Share tips, ask questions, and get advice from people who have been there.
View discussion (5 replies)