Intracranial EEG: What It Is, How It Works, and What to Expect 2026 July
Learn what an intracranial EEG test is, how it differs from standard EEG, ✅ costs, risks, and what patients can expect before, during, and after the procedure.
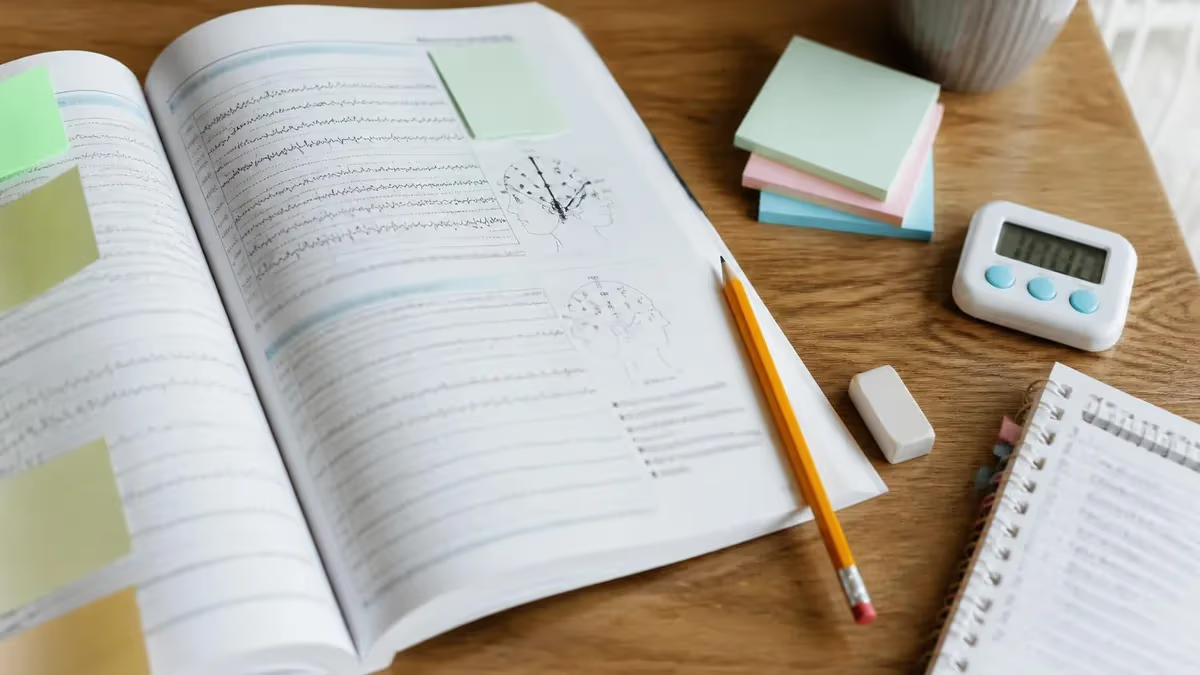
An EEG test — short for electroencephalogram — measures electrical activity in the brain by recording the signals generated by neurons firing in coordinated patterns. The standard version places electrodes on the scalp, but when doctors need far more precise data than a scalp EEG can provide, they turn to intracranial EEG, a specialized form of the intracranial eeg evaluation that places recording electrodes directly on or inside brain tissue. This technique captures seizure activity with a clarity and spatial resolution that surface recordings simply cannot match.
Intracranial EEG is most commonly ordered for patients with drug-resistant epilepsy who are being evaluated for surgical treatment. When a person has experienced multiple seizures that do not respond to two or more appropriate anti-seizure medications, neurologists begin exploring whether a discrete region of the brain is responsible for generating those seizures. Identifying that region with enough precision to guide a surgeon requires more than a scalp EEG can deliver, because bone, dura, and cerebrospinal fluid all dampen and blur the electrical signals traveling from the cortex to the scalp.
The procedure involves a neurosurgeon implanting one of several electrode types — strip electrodes, grid electrodes, or depth electrodes — in carefully selected brain regions. The patient then spends days to weeks in a dedicated epilepsy monitoring unit while seizures are recorded, mapped, and analyzed by a multidisciplinary team that includes epileptologists, neuropsychologists, and neurosurgeons. Every aspect of the EEG medical test is designed to answer a single clinical question: can we safely remove the seizure-generating region without causing unacceptable neurological deficits?
Understanding what an intracranial EEG involves matters not only for patients and families preparing for the procedure, but also for EEG technologists, neurology residents, and certification candidates who need to master the full spectrum of electroencephalography. The technical demands of recording and reviewing intracranial data are substantially different from routine scalp EEG work, requiring familiarity with high-density montages, reference strategies unique to implanted arrays, and the interpretation of local field potentials rather than volume-conducted signals.
This guide covers the full scope of intracranial EEG: the clinical indications, the types of electrodes used, the surgical implantation process, what patients experience during the monitoring phase, how clinicians interpret the data, and the risks and costs associated with the procedure. Whether you are a patient researching your upcoming evaluation, a technologist studying for credentialing, or a clinician brushing up on the latest techniques, this resource provides the depth you need to understand this powerful but demanding EEG test in full context.
Throughout this article we will also address common patient questions, including how long an EEG test of this type takes, what intracranial EEG side effects and risks look like compared to surface monitoring, and what the eeg test price landscape looks like in the United States. By the end, you will have a clear, evidence-based picture of why intracranial EEG remains the gold standard for presurgical epilepsy evaluation and what the monitoring experience actually involves for the people who undergo it.
Intracranial EEG by the Numbers
Types of Intracranial EEG Electrodes
Thin flexible arrays of 4–8 contacts placed between the brain surface and dura mater. Strips are threaded through small burr holes and cover linear regions of cortex, making them ideal for lateral or basal surfaces where grid placement is impractical.
Rectangular arrays of 16–64 contacts implanted via craniotomy. Grids cover broad cortical regions and are essential for detailed mapping of eloquent cortex — language, motor, or sensory areas — adjacent to a suspected seizure focus.
Thin, pencil-like electrodes inserted through small drill holes using robotic stereotactic guidance. SEEG reaches deep structures like the amygdala, hippocampus, and insula that grids cannot access, with lower infection risk and shorter recovery.
Semi-invasive electrodes inserted through the foramen ovale in the skull base to record from mesial temporal structures. Used when hippocampal involvement is suspected but full SEEG implantation is considered too risky for the individual patient.
Before a neurosurgeon implants any intracranial electrode, the patient undergoes an exhaustive non-invasive presurgical evaluation. This phase typically includes prolonged scalp video-EEG monitoring, high-resolution MRI with epilepsy-specific protocols, FDG-PET scanning, neuropsychological testing, and often functional MRI or magnetoencephalography. The goal is to form a hypothesis about where seizures originate and which electrode configuration will best test that hypothesis. The implantation plan is discussed in a multidisciplinary team conference where epileptologists, neurosurgeons, and neuroradiologists jointly review all available data before agreeing on electrode placement.
The surgical implantation itself is performed under general anesthesia and typically takes two to six hours depending on the number and type of electrodes being placed. For subdural grids and strips, the neurosurgeon performs a craniotomy — removing a section of skull — to access the cortical surface, places the electrodes precisely, then closes the scalp while leaving electrode wires tunneled to connectors outside the skin.
For SEEG, the approach is less invasive: a robotic system such as the ROSA or Neuromate guides drill bits through small twist-drill holes, and electrodes are advanced along pre-planned trajectories using real-time imaging feedback to avoid blood vessels.
After surgery, the patient is transferred to the epilepsy monitoring unit, where they are continuously observed by video and EEG recording. Anti-seizure medications are typically reduced or withdrawn to facilitate seizure occurrence. The monitoring team reviews EEG data in near-real time, looking for both interictal discharges — abnormal spikes that occur between seizures — and ictal activity, meaning the electrical signature of actual seizures as they begin and evolve. The spatial pattern of ictal onset across the implanted contacts defines the seizure onset zone, which is the primary surgical target.
Functional cortical mapping is another critical component of the intracranial monitoring phase, particularly when electrodes overlie eloquent cortex. Electrical stimulation is delivered through pairs of contacts while the patient performs language, motor, or sensory tasks. Areas where stimulation disrupts function are marked as eloquent and must be preserved during any subsequent resection. This mapping process can take several sessions spread across the monitoring period, adding to the overall duration of the hospital stay and the total eeg test cost.
Once enough seizures have been captured and functional mapping is complete, the electrode removal surgery is scheduled. For subdural grids and strips, removal requires a second craniotomy under general anesthesia. SEEG electrodes are removed at the bedside or in a minor procedure room under sedation, as they leave only small needle-track wounds. After electrode removal, the patient typically remains hospitalized for one to three days for observation before being discharged with a follow-up plan that includes further outpatient EEG testing and surgical planning if resection is recommended.
The entire process from implantation to discharge commonly spans ten to twenty-one days, which explains why the eeg test price for intracranial monitoring is vastly higher than a standard outpatient scalp EEG. Hospital room charges, operating room fees, neurosurgery professional fees, equipment costs, and intensive nursing care in a specialized epilepsy monitoring unit all accumulate over the monitoring period. Insurance coverage plays a major role in out-of-pocket costs, and patients are strongly advised to obtain prior authorization and understand their benefits before the procedure begins.
The data generated during intracranial monitoring is reviewed not only in real time but also in detailed offline analysis after the monitoring period ends. Quantitative EEG tools, high-frequency oscillation analysis, and spike propagation mapping help epileptologists refine their characterization of the seizure onset zone. This analysis feeds directly into the surgical planning session that follows, where the team decides whether resection, laser ablation, neurostimulation, or continued medical management is the most appropriate path forward for the individual patient.
EEG Test Cost, Duration, and What It Measures
The eeg test cost for intracranial monitoring in the United States ranges from approximately $50,000 to over $150,000 when all charges are included — surgical fees, hospital room charges, equipment, anesthesia, and specialist professional fees. Standard outpatient scalp EEG, by contrast, typically costs between $200 and $700 before insurance. The dramatic price difference reflects the complexity of neurosurgery, the specialized monitoring unit stay, and the multidisciplinary team required to manage implanted patients safely around the clock.
Most major insurers cover intracranial EEG when medically necessary criteria are met, which generally requires documentation of drug-resistant epilepsy and completion of a standard non-invasive presurgical evaluation. Prior authorization is almost always required, and patients should ask their epilepsy center's insurance coordinator to obtain written approval before scheduling. Out-of-pocket costs vary by plan but can still reach several thousand dollars even with good insurance, so understanding deductibles, out-of-pocket maximums, and in-network surgeon status is essential planning work before proceeding.
Intracranial EEG: Benefits and Drawbacks
- +Provides spatial resolution that scalp EEG cannot achieve, precisely localizing seizure onset zones
- +Enables detection of high-frequency oscillations and subtle ictal patterns invisible on surface recordings
- +Allows functional cortical mapping through direct electrical stimulation to protect eloquent areas
- +Can record from deep brain structures — amygdala, hippocampus, insula — inaccessible to scalp electrodes
- +Guides surgical planning with enough precision to achieve 60–70% seizure-free rates after resection
- +SEEG approach is minimally invasive with short recovery, low infection risk, and no craniotomy required
- −Requires neurosurgery under general anesthesia, carrying inherent surgical and anesthetic risks
- −Infection risk at electrode entry sites, though typically below 3% at experienced centers
- −Hemorrhage risk from electrode placement, particularly for depth electrodes near blood vessels
- −Total hospitalization often lasts two to three weeks, requiring extended work and family leave
- −Very high cost — $50,000 to $150,000 total — even with insurance covering the bulk of charges
- −Electrode placement is guided by a pre-existing hypothesis; if the hypothesis is wrong, the study may be non-diagnostic and need to be repeated
Pre-Procedure Checklist for Intracranial EEG Patients
- ✓Obtain written insurance pre-authorization and confirm in-network status for all surgeons and the hospital facility.
- ✓Arrange a minimum of three weeks of work or school leave to cover implantation, monitoring, and recovery.
- ✓Designate a family member or caregiver to stay available during the entire monitoring period for support and decision-making.
- ✓Complete all pre-surgical evaluations — scalp video-EEG, MRI, PET, neuropsychological testing — before the implantation date.
- ✓Discuss which anti-seizure medications will be reduced during monitoring and prepare for increased seizure frequency.
- ✓Confirm the hospital has a dedicated epilepsy monitoring unit with 24-hour nursing coverage and continuous EEG review.
- ✓Pack comfortable, loose-fitting clothing that does not need to be pulled over the head; button-front shirts are ideal.
- ✓Bring entertainment, books, and charging equipment — monitoring unit rooms restrict mobility significantly.
- ✓Ask your epileptologist to explain the decision tree: what findings would lead to resection, ablation, stimulation, or no surgery.
- ✓Schedule a post-monitoring follow-up appointment to review results and discuss the surgical planning conference outcome.
The Seizure Onset Zone Is Not Always the Same as the Lesion
MRI may identify a structural abnormality such as cortical dysplasia or a low-grade tumor, but intracranial EEG studies consistently show that the electrical seizure onset zone does not always overlap precisely with the visible lesion. In 10–25% of cases, the true onset zone is adjacent to or at a distance from the imaging abnormality, making intracranial monitoring essential even when a lesion is identified on MRI.
Interpreting intracranial EEG data is one of the most technically demanding skills in clinical neurophysiology, requiring a thorough understanding of electrode geometry, reference choices, and the physiological properties of local field potentials. Unlike scalp EEG, where the recorded signal represents the sum of electrical activity from large cortical regions, intracranial recordings reflect activity from a much smaller volume of tissue surrounding each contact. This means patterns that appear identical on scalp EEG — a rhythmic theta discharge, for example — may have completely different spatial origins and clinical significance when examined at the intracranial level.
The first step in intracranial EEG interpretation is identifying the seizure onset zone by analyzing the earliest electrical change at the start of each recorded seizure. Classic intracranial ictal onset patterns include low-voltage fast activity, often in the gamma frequency range above 30 Hz; repetitive spiking that gradually evolves in frequency and amplitude; and slow depolarization shifts at the beginning of a seizure in some mesial temporal recordings. The pattern of onset can itself carry prognostic information: low-voltage fast activity at onset is associated with better surgical outcomes than diffuse, slowly evolving patterns.
High-frequency oscillations — subdivided into ripples (80–250 Hz) and fast ripples (250–500 Hz) — have emerged as particularly important biomarkers in intracranial EEG analysis. Fast ripples in particular appear to mark pathological tissue within the seizure onset zone, and studies suggest that resecting tissue generating fast ripples is associated with improved surgical outcomes. Recording these ultra-high-frequency signals requires specialized amplifier hardware capable of sampling at 2,000 Hz or higher, which is why modern intracranial EEG systems are designed with much higher sampling rates than standard scalp EEG equipment used in routine eeg test procedures.
The irritative zone — the area generating interictal spikes between seizures — is mapped separately from the ictal onset zone. Both maps are overlaid on the patient's MRI using post-implant imaging that localizes each electrode contact in three-dimensional brain space. This process, sometimes called electrode localization, uses CT-MRI co-registration to assign stereotactic coordinates to each contact with millimeter-level accuracy. The resulting maps are the visual foundation of the surgical planning conference, where the team decides exactly which tissue to target and which to spare.
Functional mapping adds another data layer to intracranial analysis. When electrical stimulation is delivered through adjacent electrode contacts at low current intensities, clinicians can elicit or suppress specific functions depending on the cortical region being stimulated. Stimulation of motor cortex produces contralateral limb movements or tingling. Stimulation of language cortex — Broca's or Wernicke's areas — disrupts speech production or comprehension. Positive and negative mapping findings are combined into a functional cortical map that defines the margins of safe resection.
Quantitative analysis tools have transformed intracranial EEG review from a purely visual task into a data-intensive workflow. Automated spike detectors identify interictal events across hundreds of channels simultaneously, generating heat maps that show spike density by brain region. Propagation analysis tracks how ictal activity spreads from contact to contact after onset, providing information about secondary spread that is relevant to surgical planning. Some centers are now integrating machine learning algorithms to assist with seizure onset zone identification, though visual review by an experienced epileptologist remains the gold standard for clinical decision-making.
The final interpretation — the clinical report summarizing the seizure onset zone, irritative zone, eloquent cortex boundaries, and surgical recommendation — is produced by the epileptologist and presented at the multidisciplinary surgical planning conference. This report synthesizes days to weeks of continuous data recording, hundreds of hours of signal, and the integrated opinions of a team of specialists.
It is, in every sense, the culmination of the most rigorous and resource-intensive form of the EEG medical test available in contemporary neurology, and its conclusions directly determine whether a patient proceeds to surgery that may free them from years of disabling seizures.
Anti-seizure medications are often tapered or discontinued during intracranial EEG monitoring to provoke seizures. This intentionally increases seizure frequency and, in rare cases, can trigger prolonged seizures or status epilepticus. The epilepsy monitoring unit is staffed and equipped to respond immediately, but patients and families should be counseled about this risk before agreeing to proceed with intracranial monitoring.
The risks associated with intracranial EEG are real, and patients deserve a clear-eyed discussion of them before consenting to the procedure. The most serious risks are hemorrhage and infection. Hemorrhage can occur when an electrode contacts or tears a blood vessel during insertion. In SEEG implantations, vessel-avoidance planning using high-resolution MRI angiography reduces this risk substantially, and symptomatic hemorrhage rates at experienced centers are generally below 1 to 2 percent. Subdural grid implantations carry somewhat higher hemorrhage risk because the craniotomy itself involves greater tissue manipulation, but rates at high-volume epilepsy centers remain low.
Infection is the other major concern. Electrode wires exiting through the scalp create a potential pathway for bacteria, and the risk increases with longer monitoring durations. Most centers prophylactically administer antibiotics for the duration of the monitoring stay and perform daily wound care at electrode exit sites. Published infection rates at experienced centers range from 1 to 3 percent for superficial wound infections and below 1 percent for deep infections such as meningitis or abscess. Patients who develop fever or increased pain around electrode sites during monitoring should report these symptoms immediately.
Neurological deficits are a less common but important risk. Electrode placement in or near eloquent cortex can cause temporary or, rarely, permanent deficits in motor, sensory, or language function. The precise pre-operative planning that characterizes modern intracranial EEG evaluation is specifically designed to minimize this risk by routing electrode trajectories away from functional tissue whenever anatomically feasible. Nonetheless, patients should be informed that transient word-finding difficulties, limb weakness, or sensory changes are possible, particularly in the immediate postoperative period when tissue swelling is greatest.
EEG test side effects specific to the monitoring phase itself — as opposed to the surgical implantation — include headache, scalp discomfort at electrode sites, and the psychological stress of prolonged hospitalization with restricted mobility. Sleep disruption is common, both because monitoring-unit environments are inherently noisy and because nocturnal seizures may occur more frequently when medications are reduced. Patients with anxiety or claustrophobia should discuss these concerns with their care team in advance, as appropriate supportive measures — including short-term anxiolytic therapy — can be arranged.
Long-term risks after electrode removal are generally low. Most patients recover fully from both implantation and removal surgeries without lasting neurological change. The craniotomy scar from grid implantation heals over weeks to months, and SEEG entry sites are small enough to be nearly invisible at one year. The greatest long-term risk is actually not from the monitoring itself but from the subsequent resective surgery if the patient proceeds to that next step — but that risk is separate from the diagnostic intracranial EEG procedure and is evaluated independently based on the specific surgical plan.
Cost remains a significant practical concern for many patients. As noted earlier, the total eeg test cost for intracranial monitoring typically falls between $50,000 and $150,000 in the United States. Insurance covers the majority of this for patients who meet medical necessity criteria, but the out-of-pocket exposure can still be substantial. Some centers have financial counselors available to help patients navigate prior authorization, appeals, and payment plans. For uninsured or underinsured patients, academic medical centers and epilepsy research programs sometimes offer reduced-cost monitoring as part of prospective research studies, which is worth inquiring about during the initial evaluation.
Ultimately, the risk-benefit calculation for intracranial EEG must be weighed against the risks and costs of untreated drug-resistant epilepsy. Patients with uncontrolled seizures face elevated risks of sudden unexpected death in epilepsy (SUDEP), serious injury from falls, significant cognitive and psychological morbidity, and profound limitations on employment, driving, and quality of life. For carefully selected candidates, intracranial EEG is not merely a diagnostic test — it is the gateway to a potentially transformative surgical outcome that routine eeg test procedures cannot facilitate.
For EEG technologists and certification candidates, understanding intracranial EEG from a technical standpoint is increasingly important as the field expands and more monitoring centers seek credentialed staff familiar with invasive recording techniques. The R. EEG T. and CLTM examinations both include questions touching on advanced EEG methodology, electrode types, and signal characteristics that overlap with intracranial recording concepts. Even technologists who will never work in a dedicated epilepsy monitoring unit benefit from understanding how intracranial data differs from scalp data, because this knowledge deepens comprehension of why scalp EEG looks the way it does.
From a technical standpoint, intracranial recordings present several challenges that scalp EEG does not. Impedance matching is one: intracranial electrode contacts are metallic and interface directly with cerebrospinal fluid or brain tissue, producing very low impedance values — often below 5 kilohms — compared to the 5- to 10-kilohm target range for scalp electrodes. Amplifier input impedance requirements are therefore different, and technologists working with intracranial systems must understand these distinctions to troubleshoot artifact and connectivity problems effectively.
Referencing strategies in intracranial EEG are also more complex. Common average reference, linked mastoid reference, and bipolar montages are all used for scalp EEG, but in intracranial recordings, reference choice has a dramatic impact on signal appearance because nearby contacts may themselves be recording active epileptiform data.
Many centers use a reference contact placed in white matter or at a cortical location known to be outside the seizure onset zone, but there is no universally agreed-upon standard. Technologists and electroencephalographers alike must understand the effect of reference selection on waveform morphology and must be able to switch between montages fluidly during data review.
Artifact recognition in intracranial recordings includes familiar culprits — electrode movement, cardiac artifact, EMG — as well as sources unique to implanted arrays. Cerebrospinal fluid pulsation produces a rhythmic artifact in some subdural recordings. Stimulation artifact from functional mapping sessions creates high-amplitude transients that must be recognized and excluded from quantitative analyses. And the physical proximity of electrode contacts to each other can produce capacitive coupling artifacts in bipolar montages that mimic high-frequency oscillations if not carefully distinguished from genuine neural signals.
Study strategies for certification candidates covering intracranial EEG topics should include reviewing the ACNS guidelines on invasive EEG monitoring, reading foundational journal articles on SEEG technique and intracranial signal interpretation, and working through practice questions that test conceptual understanding rather than rote memorization. The principles underlying intracranial EEG — spatial sampling, signal-to-noise ratio, reference effects, frequency content — apply directly to scalp EEG interpretation and will strengthen your overall performance on any EEG certification examination.
Practice tests are one of the most effective preparation tools available. Working through questions on abnormal epileptiform patterns, activation procedures, and ambulatory EEG builds the pattern recognition skills that experienced electroencephalographers develop over years of clinical practice. Each practice session reinforces the underlying physiological concepts and exposes gaps in knowledge that can then be targeted with focused review. The quiz resources linked throughout this article are specifically designed for EEG certification preparation and cover the full range of topics likely to appear on credentialing examinations.
Whether you are preparing for a credentialing exam, counseling a patient about their upcoming procedure, or managing an epilepsy monitoring unit, the knowledge foundation built around intracranial EEG extends your understanding of the entire field of electroencephalography. The extreme precision of intracranial recording illuminates the physiological basis of every EEG pattern you will see in clinical practice, from the simplest alpha rhythm to the most complex ictal discharge. Investing in this understanding pays dividends across every context in which you engage with the EEG test in your professional or patient life.
EEG Questions and Answers

EEG vs ECG vs EKG: Brain and Heart Test Differences

EEG Electroencephalography Practice Test PDF (Free Printable 2026)

What Does an EEG Measure? Brain Waves, Electrical Activity, and What Your Results Reveal

How to Read an EEG Test: A Complete Guide to Brain Wave Patterns and Results

EEG Waves Explained: Delta, Theta, Alpha, Beta, and Gamma Brain Rhythms
About the Author

Educational Psychologist & Academic Test Preparation Expert
Columbia University Teachers CollegeDr. Lisa Patel holds a Doctorate in Education from Columbia University Teachers College and has spent 17 years researching standardized test design and academic assessment. She has developed preparation programs for SAT, ACT, GRE, LSAT, UCAT, and numerous professional licensing exams, helping students of all backgrounds achieve their target scores.