EEG Equipment Guide: Machines, Electrodes, Costs, and What Patients Should Know
Complete guide to EEG equipment: machines, electrodes, amplifiers, costs, and how the eeg test works for patients and technicians. 📝

An eeg test relies on a surprisingly intricate stack of EEG equipment — from the soft caps that hug a patient's scalp to the multi-channel amplifiers that translate microvolt brain signals into the squiggly traces neurologists read. If you have an EEG scheduled, are studying to become a technologist, or run a clinic considering a new system, understanding the gear matters. The right setup directly affects recording quality, patient comfort, technician workflow, and ultimately, the diagnostic confidence a physician can place in the final report.
Modern EEG equipment looks very different from the paper-strip machines of the 1990s. Today's clinical systems are mostly digital, with 32 to 256 channels, video synchronization, ambulatory recorders the size of a paperback book, and software that can flag spikes, seizures, and artifacts in near real time. Even so, the fundamentals haven't changed: silver–silver chloride electrodes, conductive paste or gel, and a careful 10-20 placement scheme still form the backbone of nearly every routine and long-term study.
This guide walks through every major category of EEG hardware and software you're likely to encounter. We'll cover the headboxes and amplifiers that capture signal, the electrodes and caps that bridge skin to silicon, the impedance meters that quietly determine whether your recording is clean or full of noise, and the review workstations where the actual interpretation happens. We'll also break down what EEG equipment costs in 2026 — for individual electrodes, for full clinical systems, and for the rapidly growing consumer wearables segment.
Patients usually have one practical question: what does this stuff feel like, and is any of it risky? The short answer is that standard EEG equipment is completely non-invasive. Nothing transmits current into your brain; the system only listens. The paste washes out, the electrodes leave no marks, and the worst inconvenience is usually sticky hair for a few hours afterward. There are no needles, no radiation, and no contrast injection — unlike CT or MRI scans.
For clinicians and EEG technologists, equipment selection is more nuanced. A pediatric epilepsy monitoring unit needs different gear than a sleep lab or an ICU continuous monitoring service. Ambulatory recorders sacrifice channel count for portability. Research labs may push to 256 high-density channels to localize sources millimeter by millimeter. We'll work through these trade-offs so you can match equipment to clinical purpose rather than chasing specs.
By the end of this article you should know how to identify the parts of an EEG machine, what each component does, what a routine EEG test costs in the US, how long studies typically last, what side effects to expect (spoiler: very few), and how to evaluate hardware if you're buying or specifying a system. We'll also link out to deeper articles on EEG waveforms, ambulatory studies, and tech career paths if you want to go further on any single topic.
Whether you're a curious patient, a student preparing for boards, or a department lead writing a capital request, this is the practical, technology-focused reference we wish more EEG sites had.
EEG Equipment by the Numbers
Core EEG Equipment Components
The small input device that electrodes plug into. It pre-amplifies microvolt signals and digitizes them before sending to the recording computer, minimizing noise pickup along the cable run.
Silver–silver chloride electrodes attached to the scalp with conductive paste, glue, or worn inside an elastic cap. They detect the tiny electrical fields generated by cortical neurons.
A medical-grade PC running EEG software that displays live tracings, manages photic and hyperventilation activation, and stores the study for later review and reporting.
Built into modern amplifiers, it measures skin-electrode contact quality in kilo-ohms. Anything under 5 kΩ is ideal; readings above 10 kΩ usually mean re-prepping the site.
A strobe lamp drives photic activation up to 30 Hz to provoke abnormalities, while a synchronized HD camera captures patient behavior for later video-EEG correlation.
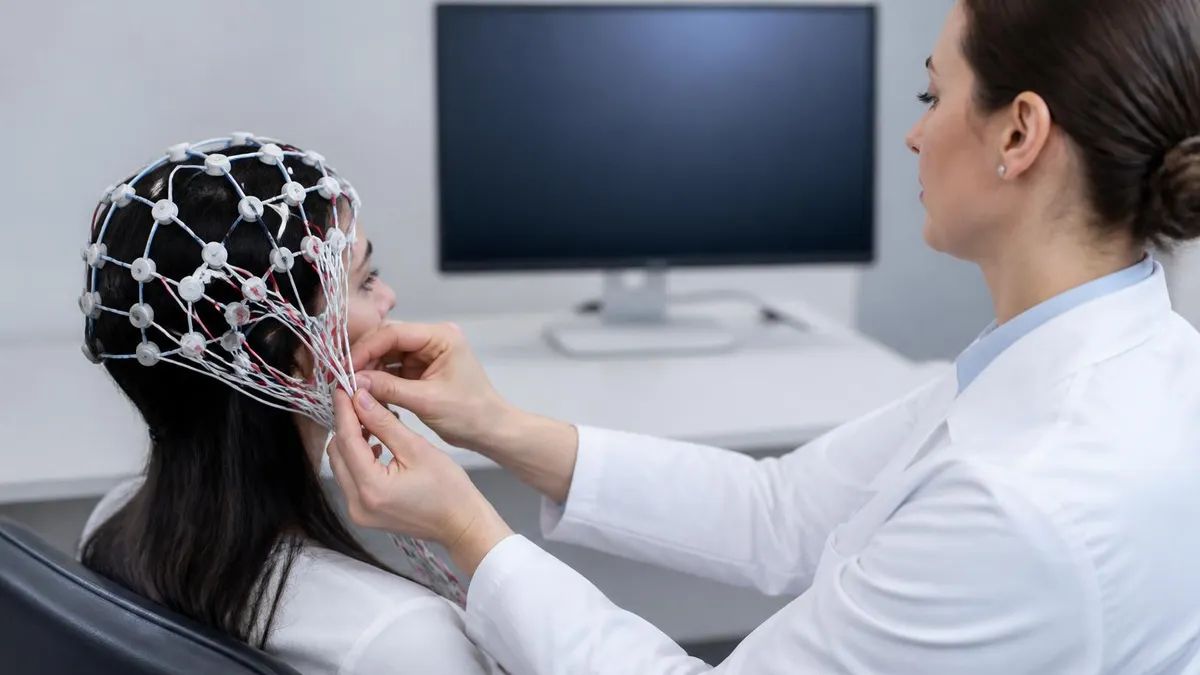
Electrodes are where EEG begins. Every signal you ever see on a tracing started as a few microvolts of voltage difference measured between two silver–silver chloride pellets touching the scalp. Because the signals are so small — about a million times weaker than a standard household outlet — everything downstream is essentially a war against noise.
That war is won or lost at the electrode site, which is why technologists spend so much time prepping the skin with abrasive gel before applying conductive paste. If you're new to interpretation, our reference on what is an eeg test shows how clean recordings translate into clinically meaningful waveforms.
The international 10-20 system standardizes where each electrode goes. The name refers to the proportional distances — 10% or 20% of the total skull measurement — between adjacent electrodes. A routine clinical montage uses 21 electrodes labeled by region: Fp (frontopolar), F (frontal), C (central), P (parietal), O (occipital), T (temporal), plus the midline Fz, Cz, and Pz. Odd numbers sit on the left, even numbers on the right, and 'z' marks the midline. Once you learn the pattern, reading any montage becomes much easier.
For long-term monitoring or research, technologists may upgrade to a 10-10 or 10-5 layout, expanding the electrode count to 64, 128, or even 256. High-density arrays improve spatial resolution and source localization, which matters for pre-surgical epilepsy evaluations where neurologists are trying to pinpoint a seizure-onset zone. The trade-off is setup time: a 256-channel cap might take 45 to 90 minutes to apply properly, versus 20 minutes for a routine 21-channel study.
Cap-based systems use an elastic mesh with electrodes pre-positioned at standard locations. The technologist parts hair, injects conductive gel through a small hole in each electrode housing, and checks impedance. Cap systems are faster and more reproducible across patients, which is why most sleep labs, ICUs, and ambulatory services prefer them. However, individual disc electrodes glued with collodion are still standard for long-term inpatient epilepsy monitoring, where electrodes need to stay attached for 5 to 10 days.
Reference and ground electrodes deserve special mention. Most clinical systems use a linked-ears or average reference, though some prefer Cz or a contralateral mastoid. The ground electrode — usually on the forehead — gives the amplifier a common voltage baseline. Without a properly placed ground, you'll see massive 60 Hz line noise drowning out brain activity. Trainees often underestimate how much of a clean recording depends on these two 'non-recording' electrodes.
Beyond the scalp, ancillary electrodes capture artifacts and physiological correlates. EOG electrodes near the eyes detect blinks and saccades. EMG leads on the chin or limbs flag muscle tension and movement. ECG from a single chest lead helps distinguish cardiac artifact from sharp transients. In sleep studies, respiratory belts, oximetry, and airflow sensors round out the polysomnography montage. EEG equipment is rarely just about brain signal — it's an integrated multi-modal recording system.
Finally, electrode hygiene matters. Disposable single-use electrodes are common in ICUs to prevent infection. Reusable silver-silver chloride electrodes must be cleaned with enzymatic detergent and re-chlorided periodically, or impedance drifts upward and signal quality drops. Many EEG labs maintain a logbook for electrode life cycles, and any tech who has chased mystery artifact for an hour learns quickly that worn electrodes are a top-three suspect.

EEG Practice Test Questions
Prepare for the EEG - Electroencephalography exam with our free practice test modules. Each quiz covers key topics to help you pass on your first try.
EEG Abnormal Epileptiform Patterns
EEG Exam Questions covering Abnormal Epileptiform Patterns. Master EEG Test concepts for certification prep.
EEG Activation Procedures
Free EEG Practice Test featuring Activation Procedures. Improve your EEG Exam score with mock test prep.
EEG Artifact Identification
EEG Test Prep for Artifact Identification. Practice EEG Quiz questions and boost your score.
EEG Electrode Placement and Montages
EEG Questions and Answers on Electrode Placement and Montages. Free EEG practice for exam readiness.
EEG - Electroencephalography Abnormal Epil...
EEG Mock Test covering - Electroencephalography Abnormal Epileptiform Patterns. Online EEG Test practice with instant feedback.
EEG - Electroencephalography Activation Pr...
Free EEG Quiz on - Electroencephalography Activation Procedures. EEG Exam prep questions with detailed explanations.
EEG - Electroencephalography Artifact Iden...
EEG Practice Questions for - Electroencephalography Artifact Identification. Build confidence for your EEG certification exam.
EEG - Electroencephalography Electrode Pla...
EEG Test Online for - Electroencephalography Electrode Placement and Montages. Free practice with instant results and feedback.
EEG - Electroencephalography Instrumentati...
EEG Study Material on - Electroencephalography Instrumentation and Calibration. Prepare effectively with real exam-style questions.
EEG - Electroencephalography Neuroanatomy ...
Free EEG Test covering - Electroencephalography Neuroanatomy and Physiology. Practice and track your EEG exam readiness.
EEG - Electroencephalography Non-Epileptif...
EEG Exam Questions covering - Electroencephalography Non-Epileptiform Abnormalities. Master EEG Test concepts for certification prep.
EEG - Electroencephalography Normal EEG Wa...
Free EEG Practice Test featuring - Electroencephalography Normal EEG Waveforms. Improve your EEG Exam score with mock test prep.
EEG - Electroencephalography Patient Safet...
EEG Mock Exam on - Electroencephalography Patient Safety and Ethics. EEG Study Guide questions to pass on your first try.
EEG - Electroencephalography Pediatric and...
EEG Test Prep for - Electroencephalography Pediatric and Neonatal EEG. Practice EEG Quiz questions and boost your score.
EEG ICU and Continuous EEG Monitoring
EEG Questions and Answers on ICU and Continuous EEG Monitoring. Free EEG practice for exam readiness.
EEG Instrumentation and Calibration
EEG Mock Test covering Instrumentation and Calibration. Online EEG Test practice with instant feedback.
EEG Neuroanatomy and Physiology
Free EEG Quiz on Neuroanatomy and Physiology. EEG Exam prep questions with detailed explanations.
EEG Non-Epileptiform Abnormalities
EEG Practice Questions for Non-Epileptiform Abnormalities. Build confidence for your EEG certification exam.
EEG Normal EEG Waveforms
EEG Test Online for Normal EEG Waveforms. Free practice with instant results and feedback.
EEG Patient Safety and Ethics
EEG Study Material on Patient Safety and Ethics. Prepare effectively with real exam-style questions.
What Is an EEG Medical Test?
A routine EEG is the standard outpatient electroencephalogram, lasting 20 to 40 minutes after setup. The technologist applies 21 scalp electrodes, records baseline activity, then runs activation procedures: hyperventilation for three minutes and photic stimulation through a series of flash frequencies. Patients lie quietly with eyes alternately open and closed.
This study is the workhorse for evaluating new-onset seizures, episodes of altered awareness, and unexplained syncope. It captures only a small slice of brain activity, so a normal routine EEG never fully rules out epilepsy. Sensitivity for detecting interictal abnormalities in known epilepsy patients sits around 50% on a first study and rises with sleep-deprived or repeated recordings.
EEG Equipment: Clinical Pros and Cons
- +Completely non-invasive — no needles, radiation, or contrast
- +Excellent temporal resolution — millisecond-level brain activity tracking
- +Relatively low cost compared to MRI or PET imaging
- +Portable systems enable ICU bedside and home ambulatory recording
- +Safe for children, pregnant patients, and people with implants
- +Real-time spike and seizure detection software is widely available
- +Reusable electrodes keep per-patient consumable costs low
- −Limited spatial resolution — cannot localize deep brain structures
- −Highly susceptible to muscle, eye-blink, and line-noise artifacts
- −Setup requires skilled technologists and proper skin preparation
- −Sticky paste and gel can leave hair messy for hours
- −Routine studies have only ~50% sensitivity in known epilepsy
- −High-density systems require long setup and significant data storage
EEG Equipment Setup Checklist for Technologists
- ✓Verify amplifier, cables, and electrode integrity before patient arrival
- ✓Confirm patient identity, study type, and any medication holds
- ✓Measure head circumference and mark 10-20 positions accurately
- ✓Clean each scalp site with abrasive prep gel to reduce impedance
- ✓Apply electrodes and verify all impedances are below 5 kΩ
- ✓Place ground and reference electrodes correctly to suppress line noise
- ✓Document calibration, biocalibration, and montage selection
- ✓Position photic stimulator at 30 cm and test all flash frequencies
- ✓Synchronize video, audio, and patient event button before recording
- ✓Annotate hyperventilation, eye opening, and any clinical events live
Keep every electrode under 5 kΩ before recording starts
Most artifact problems trace back to a single bad electrode. Spending five extra minutes to re-prep a site that's reading 12 kΩ will save you an hour of review-side cleanup — and may save a study from being declared non-diagnostic. Impedance equality across electrodes is nearly as important as absolute values: mismatched contacts amplify common-mode noise like 60 Hz hum.
What does an eeg test price look like in the US in 2026? The honest answer is 'it depends,' but we can give you concrete ranges. A routine outpatient EEG billed under CPT 95816 or 95819 typically lists at $400 to $1,200 before insurance adjustments. After commercial insurance contracts, your responsibility is usually $40 to $300 depending on your deductible, copay, and whether the facility is in-network. Medicare reimburses providers roughly $90 to $180 for a routine study, which sets a floor that most commercial plans negotiate against.
Ambulatory EEGs are pricier because of the longer recording, equipment rental, and technologist time on both ends. Expect list prices of $1,500 to $3,500 for a 24- to 72-hour study, with patient out-of-pocket landing between $200 and $1,200 after insurance. CPT codes 95705 through 95711 cover the various ambulatory configurations — with and without video, with and without technologist review. Make sure you understand which specific code your provider plans to bill, because reimbursement varies widely.
Inpatient long-term video-EEG monitoring is by far the most expensive format. A 5-day EMU admission can easily run $15,000 to $50,000 in total facility and professional charges, particularly at academic epilepsy centers. Insurance generally covers this when medically necessary, but patients still face hospital deductibles, daily inpatient copays, and surprise out-of-network professional bills. Ask for a written cost estimate before admission whenever possible.
For practices buying equipment, a complete clinical EEG system — amplifier, software, two acquisition stations, electrode supplies for 6 months, and training — typically runs $35,000 to $80,000. High-density research systems with 128 to 256 channels can exceed $150,000. Ambulatory recorders are sold individually at $8,000 to $15,000 per unit, and most labs need at least three to four to keep their schedule running smoothly. Service contracts add 8 to 12% of system cost annually.
Per-study consumables are surprisingly small. Disposable electrodes cost about $1 to $3 each, conductive paste runs $30 to $50 per jar, and abrasive prep gel is a few dollars per tube. Skin-marking pencils, gauze, and head wraps add another dollar or two. Even at the high end, total consumables for a single routine study sit under $20. The dominant cost driver is always technologist labor — typically 60 to 75% of the study's true cost.
For patients, the most useful cost-saving step is to ask whether your study is being read in-house or sent to an outside neurologist. Both options can result in two separate bills: one for the technical (facility) component and one for the professional (interpretation) component. Confirming both providers are in-network can reduce a $1,500 bill to a $250 bill. It's the single most under-publicized billing tip in neurodiagnostics.
Finally, if you're paying cash, many outpatient clinics offer 25 to 50% discounts for upfront payment. A routine EEG that lists at $900 might drop to $400 with a self-pay rate. Ambulatory studies sometimes price as low as $750 cash at independent diagnostic facilities. Always ask — most billing departments will quote you a discount if you ask in writing before the study.
Avoid conditioner, oils, hairspray, or styling products on the day of your EEG — they form an insulating film that drives electrode impedance up and degrades signal quality. Clean, dry hair with no product is ideal. Skip caffeine for 8 hours unless your doctor specifically requested otherwise, and bring a list of current medications so the technologist can document them in the record.
Patients almost always want to know two things: what is eeg test like in terms of duration, and what side effects to expect. Both answers are reassuring. A routine outpatient EEG, from check-in to walking out the door, typically takes 60 to 90 minutes. The recording itself runs 20 to 40 minutes; the rest is setup, activation procedures, and electrode removal. Sleep-deprived EEGs can stretch to 90 minutes of recording. Ambulatory studies last 24, 48, or 72 hours but only require about 45 minutes of in-clinic setup at the start.
Side effects from a standard EEG are minimal because nothing is being put into your body. The most common complaints are skin irritation from prep gel (usually mild redness that fades in a few hours), sticky residue from paste that takes a shampoo or two to fully wash out, and rarely, a small abrasion if prep was overly aggressive. Patients with sensitive scalps or fresh scars should mention this beforehand so the technologist can adjust technique.
Photic stimulation deserves a special note. The strobe used during activation procedures can occasionally trigger a seizure in people with photosensitive epilepsy — which is, in part, what the test is designed to detect. If a seizure occurs, the technologist immediately stops the strobe, ensures patient safety, and continues recording to capture the event. The seizure itself is not caused by the EEG equipment; the strobe simply provokes activity that was already latent in the brain.
Hyperventilation can produce lightheadedness, tingling in the hands, or a brief feeling of anxiety. These are normal physiologic responses to the rapid breathing protocol and resolve within a minute or two of resuming normal respiration. Patients with significant cardiopulmonary disease, recent stroke, or sickle cell disease are typically excused from hyperventilation, as the cerebral vasoconstriction it produces could be harmful.
Long-term inpatient monitoring carries a slightly higher risk profile because anti-seizure medications are often tapered to provoke events. Patients in the EMU may have more seizures than they would at home, which is the whole point — but it also means injury risk from falls, status epilepticus, and post-ictal confusion must be carefully managed by trained nursing staff. EMUs are designed with padded walls, low beds, and continuous video observation specifically for this reason.
Skin breakdown can occur during multi-day recordings, especially in elderly patients or those with diabetes. Technologists check electrode sites at least once per shift and rotate any electrode showing pressure damage. Collodion-glued electrodes are removed with acetone-based solvent at the end of the study; the smell is strong but brief, and the chemical itself is FDA-approved for medical use.
For children, parents often worry about whether the test will hurt. It doesn't. The gentlest part of any pediatric EEG service is the technologist's bedside manner — they're typically experts at distraction, narrating each step, letting kids touch the cap, and making the whole experience feel like a science project rather than a medical procedure. Most children tolerate the study without sedation, even toddlers.
If you're preparing to buy, specify, or operate EEG equipment, a few practical lessons separate successful programs from frustrated ones. First, prioritize amplifier quality and software ergonomics over raw channel count. A reliable 32-channel system that a technologist actually enjoys using produces more diagnostic studies than a 256-channel showpiece that sits idle because setup takes too long. Capability that goes unused is wasted capital.
Second, plan electrode supply chains carefully. Disposable electrodes have moved through multiple shortages since 2020, and labs that depend on a single supplier have been forced to cancel studies. Maintain a 90-day buffer of consumables, qualify a second supplier where possible, and standardize on electrode types across your fleet to keep training simple and inventory predictable.
Third, invest in technologist training and retention. The single largest determinant of study quality isn't the equipment — it's the human running it. Certified technologists (R. EEG T. or CLTM credentials) command higher salaries but produce dramatically fewer non-diagnostic studies, fewer artifact-laden recordings, and shorter physician review times. The math almost always favors hiring credentialed staff and paying competitively.
Fourth, integrate EEG data with your EHR and PACS systems from day one. Studies that live on isolated workstations create chart-completion problems, billing delays, and lost data when hardware fails. Most modern EEG vendors offer HL7 and DICOM gateways; configure these properly during installation rather than trying to retrofit later. Reporting workflows that auto-populate the EHR can shave 30 minutes off every interpretation.
Fifth, take patient education seriously. A patient who understands what's happening, why the paste is sticky, and why hyperventilation makes them lightheaded is a calmer patient with cleaner data. Print a one-page prep sheet, send a confirmation email the night before, and have the technologist explain each activation procedure before starting. Five minutes of communication eliminates most artifact from anxiety and muscle tension.
Sixth, audit your equipment routinely. Run weekly calibration checks, monthly impedance verification across all amplifiers, and quarterly biocalibration drills with staff. Document everything. When the Joint Commission, CMS, or your accreditation body asks about quality assurance, you'll have a record that shows you take signal integrity seriously — and you'll catch slow-drift problems before they corrupt a year's worth of studies.
Finally, stay current. EEG equipment is evolving quickly — dry electrodes, wireless caps, automated seizure detection, cloud-based review platforms, and AI-assisted reading are all maturing fast. None of these replace fundamentals, but each can deliver real efficiency gains when matched to the right clinical use case. Subscribe to ACNS guidelines, attend an annual neurodiagnostic conference, and budget for one major equipment refresh every 5 to 7 years.
EEG Questions and Answers

EEG Tech Salary 2026: Pay by State, Experience, and Certification
EEG Tech Jobs in 2026: Career Paths, Salaries, and How to Get Hired

Reading EEG Patterns: A Practical Reference for Techs and Trainees

EEG Waves Explained: Delta, Theta, Alpha, Beta, and Gamma Brain Rhythms

Ambulatory EEG: 24-72 Hour Home Recording for Suspected Seizures
About the Author
Educational Psychologist & Academic Test Preparation Expert
Columbia University Teachers CollegeDr. Lisa Patel holds a Doctorate in Education from Columbia University Teachers College and has spent 17 years researching standardized test design and academic assessment. She has developed preparation programs for SAT, ACT, GRE, LSAT, UCAT, and numerous professional licensing exams, helping students of all backgrounds achieve their target scores.