Reading EEG Patterns: A Practical Reference for Techs and Trainees 2026 July
⏳ Reference for normal and abnormal EEG patterns: alpha, theta, sleep stages, burst suppression, spike-and-wave, phase reversal, and clinical entities.

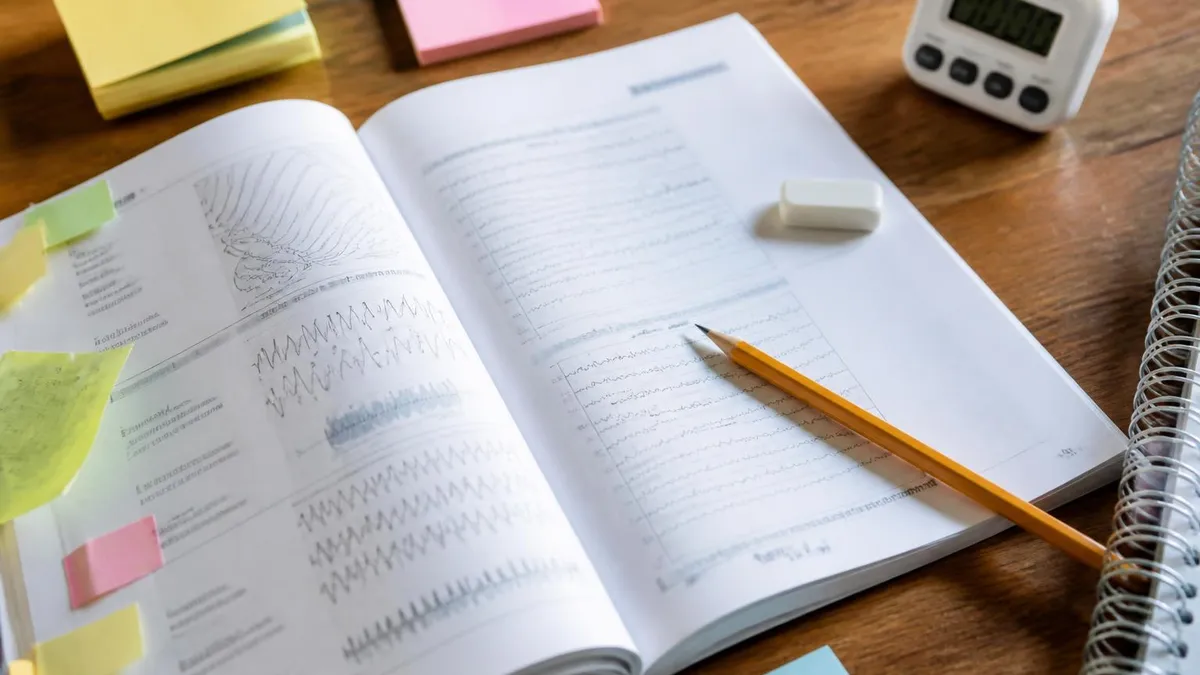
Reading an EEG is part pattern recognition and part context. The same squiggle on a screen can be a healthy alpha rhythm in a relaxed adult, or the first hint of something far less benign. New technologists often try to memorize textbook examples and then panic when a real recording looks nothing like the picture.
That reaction is normal. Real EEG is noisy, the patient blinks, the wires move, and the patterns blend into one another. This guide walks through the patterns you will actually see on shift, why they matter, and how to tell them apart without second-guessing every page.
The structure here mirrors how a working tech reads a study. We start with the baseline question, is this a normal awake recording, then move into drowsiness and sleep, and finally into the abnormal patterns that get flagged for the neurologist. Each section pairs the visual signature with the clinical meaning, because you cannot describe what you do not understand. If you are preparing for the ABRET R. EEG T. or CLTM exam, the same patterns appear on the written and practical sections, so the time you spend here pays off twice.
One ground rule before we go further. Patterns do not exist in isolation. Frequency, amplitude, location, reactivity, and symmetry all matter, and changing any one of them can flip a finding from normal variant to abnormal. Read the whole montage, not a single channel. That is the difference between a technologist who passes the boards and one who quietly catches a status epilepticus at 3 a.m.
EEG Frequency Bands at a Glance
What a normal awake and alert EEG looks like
Start with the easy one. An awake and alert adult, eyes closed, comfortable in the chair, should produce a posterior dominant rhythm in the alpha range, somewhere between 8 and 13 Hz. You will see it strongest over the occipital leads, O1 and O2, with smaller spread forward toward parietal channels. Open the eyes and the alpha attenuates within a second or two. That reactivity check is one of the first things you do on every recording, and a sluggish or absent response can be the earliest sign that something is off.
Frontally, expect low-voltage beta activity above 13 Hz, often faster and lower amplitude than the posterior alpha. Beta is the background hum of an alert cortex, and it tends to be more prominent in patients on benzodiazepines or barbiturates.
Mu rhythm, a 7 to 11 Hz arc-shaped pattern over the central regions, can show up in relaxed adults and attenuates with movement of the contralateral limb rather than eye opening. Beginners sometimes mistake mu for alpha. The trick is location and reactivity. Alpha lives at the back and responds to vision, mu lives over the motor strip and responds to movement.
Symmetry matters as much as frequency. A small persistent asymmetry, where one side runs consistently slower or lower in amplitude, can point to an underlying structural lesion long before imaging confirms it. Do not chase millivolt differences, but a clear 50 percent amplitude drop on one hemisphere deserves a note for the reader.
The alpha squeak and what it tells you
Right at eye closure many patients show a brief burst of faster alpha, often a hertz or two above their resting frequency, before the rhythm settles. This is the alpha squeak, and it is a normal finding. Flag it in your notes so a reader does not mistake the transient for a pathologic discharge. Its absence in someone who used to have one is more clinically interesting than its presence. Other normal variants in the same family include lambda waves over the occipital region during visual scanning, positive occipital sharp transients of sleep, and benign epileptiform transients of sleep, all of which can fool a newer reader if the context is missed.
Drowsiness and the slide into sleep
As the patient gets sleepy the EEG starts to change in a predictable order, and learning that order is half of staging sleep. The first sign is usually a slowing and fragmentation of the posterior alpha. Instead of running steadily it comes and goes, drops a hertz or two, and the eyes show slow rolling lateral movements rather than the sharp blinks of wake. Frontal theta in the 4 to 7 Hz range starts to creep in, and vertex sharp waves, single negative deflections at Cz, begin to appear.
This is stage N1, the lightest sleep, and patients can be roused easily. Tell a tech you are about to clap and watch the trace. Even a sleeping subject in N1 will show an arousal response. Move into N2 and the picture changes. Sleep spindles, 11 to 16 Hz bursts lasting at least half a second, ride on a slower background, and K-complexes, large biphasic transients, punctuate the record. By N3 the trace is dominated by high-amplitude delta below 4 Hz, the slow-wave sleep that pediatric techs see in the deepest part of an overnight study.
REM sleep is the strange one. The background looks almost like wake again, low-voltage and mixed-frequency, but the patient is profoundly atonic. Sawtooth waves, triangular 2 to 6 Hz runs over central leads, often herald a REM period, especially in younger patients. If you see sawtooth waves in a patient who you thought was awake, look at the chin EMG before you call it.
Sleep Stage Signatures
Alpha drops out, frontal theta appears, vertex sharp waves at Cz, slow rolling eye movements. Easiest stage to misread as drowsy wake, especially in older patients with low-voltage backgrounds. Arousal threshold is low.
Sleep spindles (11-16 Hz, >=0.5s) and K-complexes on a theta background. Defines the bulk of a normal night. Spindle morphology and density vary by age, with denser spindles in younger patients.
Slow-wave sleep, high-amplitude delta dominates >20% of an epoch. Hardest to rouse, big restorative payoff. Front-dominant slow oscillation visible at Fp1 and Fp2 channels.
Low-voltage mixed frequency, sawtooth waves, atonia on chin EMG, rapid eye movements visible on EOG channels. Dreams live here. Loss of REM atonia raises concern for REM sleep behavior disorder.
Posterior alpha rhythm 8-13 Hz, frontal beta, symmetric across hemispheres. Attenuates with eye opening within one or two seconds. Baseline for every routine recording.
Mix of alpha fragmentation, theta intrusion, and slow lateral eye movements. Not a formal stage but the transition zone where vertex waves first appear and arousal patterns are easiest to confuse.
Abnormal patterns you need to recognize on sight
Abnormal does not always mean dramatic. Some of the most clinically important findings are subtle, a single sharp wave repeating every few seconds over the same channel, a slow focal asymmetry that nobody noticed until the second hour. Others are obvious to anyone in the room. Below are the patterns most often tested on boards and most often missed in practice.
Spikes and sharp waves on EEG
A spike is a transient discharge under 70 milliseconds in duration, sharply contoured, that stands out clearly from background. A sharp wave is the slower cousin, 70 to 200 milliseconds. Both are markers of cortical irritability and, when they recur over the same area, of an epileptogenic focus. Random isolated sharps in a sleepy patient are common and rarely pathologic by themselves. Repetitive focal sharps with consistent morphology, electric field, and after-going slow wave are the ones that buy a patient a longer monitoring order.
Spike and wave discharges
The classic generalized spike-and-wave complex runs at 3 Hz, lasts a few seconds, and is the EEG signature of childhood absence epilepsy. Hyperventilation will often pull it out of a patient who looks otherwise normal at rest. Polyspike-and-wave at 4 to 6 Hz suggests juvenile myoclonic epilepsy, especially when bursts cluster on awakening. Slow spike-and-wave at 1.5 to 2.5 Hz is one of the hallmark patterns of Lennox-Gastaut syndrome. The frequency matters because it changes the differential.
Phase reversal on EEG
Phase reversal is not a pathology in itself, it is a localizing tool. In a bipolar montage, when two adjacent channels point toward each other across a common electrode, the deflections cancel at the maximum and produce an opposing waveform. That crossover electrode sits over the dipole, in other words, over the source of the discharge. If F7-T3 deflects up and T3-T5 deflects down, T3 is your focus. New techs sometimes panic at the term, but it is just geometry. Master it once and localizing focal spikes becomes routine.
Common Epileptiform Patterns Side by Side
Generalized, symmetric, frontally maximal, runs at exactly 3 Hz for a few seconds. Provoked by hyperventilation. Patient stares for a few seconds and resumes activity. Classic in childhood absence epilepsy. Background between bursts is otherwise normal, which is part of what makes the diagnosis. Watch closely for subtle eye flutter or automatisms during a run, those clinical features are usually charted by the tech in the room.
Burst suppression and what it means for the patient
Few patterns make a room go quiet faster than the first burst-suppression epoch on a fresh ICU recording. Burst suppression is exactly what it sounds like, bursts of mixed-frequency activity, often sharply contoured and high in amplitude, separated by stretches of near-flat background lasting at least a second. The ratio of burst to suppression varies, and most reading conventions ask you to estimate suppression percentage every 10 to 30 seconds.
The clinical contexts are limited and they all matter. Anesthetic burst suppression, induced by propofol, pentobarbital, or isoflurane, is a therapeutic endpoint in refractory status epilepticus, the team wants suppression because cortical activity has to be silenced for the brain to reset. Hypothermic burst suppression after cardiac arrest is part of the post-arrest care bundle. And pathologic burst suppression in a normothermic, unsedated patient is bad news, it reflects diffuse cortical injury and carries a poor prognosis, especially when bursts are stereotyped and reactivity is lost.
Document three things on every burst-suppression record, the suppression ratio, the burst morphology including any embedded epileptiform discharges, and reactivity to stimulation. A burst-suppression pattern that breaks up with a sternal rub is biologically different from one that does not flinch.
The same waveform can mean a working anesthetic, a successful cooling protocol, or a devastated cortex. Always pair the pattern with sedation history, temperature, and clinical context before you let the visual signature drive an interpretation. A note to the reader that says burst suppression, propofol at 80 mcg/kg/min, last bolus 10 minutes ago tells a different story than the same waveform on no sedation, day three post arrest. Document reactivity to sternal rub on every burst-suppression record.
Specific clinical patterns worth memorizing
Some patterns are rare enough that you may go a year without seeing one, and recognizable enough that missing one feels like a personal failure. These are the ones that show up on boards and on every senior technologist's mental greatest hits list.
Extreme delta brush on EEG
Extreme delta brush is a striking pattern, slow delta waves in the 1 to 3 Hz range with superimposed faster beta activity riding on top like surf on a wave. It looks busy and chaotic. The clinical association is what makes it special. Extreme delta brush appears in roughly 30 percent of patients with anti-NMDA receptor encephalitis and is unusual in other contexts.
If you see it in a young woman with new-onset psychiatric symptoms and dyskinesias, the team should already be drawing antibody titers. The pattern can persist for weeks and tends to resolve as the patient improves, which makes it useful for monitoring treatment response.
Alpha coma EEG pattern
Alpha coma is one of the great cognitive traps in EEG reading. The trace looks like a normal awake background, alpha in the posterior leads, but the patient is comatose and the rhythm does not attenuate to eye opening, sound, or pain. Reactivity is the giveaway. Causes include post-cardiac-arrest anoxic injury, brainstem stroke, and certain drug toxicities. Prognosis is generally poor when alpha coma follows hypoxic injury, better when it follows pontine stroke. The morphology can look reassuring at first glance, which is why a careful reactivity check on every comatose patient is non-negotiable.
Ciganek rhythm and other midline variants
Ciganek rhythm, also called midline theta of Ciganek, is a 5 to 7 Hz monomorphic rhythm at the vertex, often with a sharp or arcuate contour, seen mostly in adolescents and young adults during drowsiness. It can look alarming if you have never met it before. It is a normal variant. The key is location at the midline central electrode, the reactivity to alerting, and the absence of after-going slow wave or clinical correlate. Misreading it as epileptiform is a known board trap and a known clinical embarrassment.
Pre-Call Verification Checklist
- ✓Confirm the transient is sharply contoured and clearly stands out from the surrounding ongoing background activity
- ✓Verify the duration falls within spike or sharp wave range, not a brief artifact spike from movement or electrode pop
- ✓Check for an after-going slow wave, the classic spike plus slow wave morphology that defines an epileptiform discharge
- ✓Localize the field across multiple electrodes, a true cortical discharge has a logical spread that respects scalp geometry
- ✓Look for phase reversal in a bipolar montage to pin down the source electrode over the underlying dipole
- ✓Rule out the usual artifact sources, electrode pop, sweat sway, ECG contamination, muscle bursts, and eye movements
- ✓Compare morphology to other transients across the record, real discharges repeat with consistent shape and field
- ✓Document state, sleep stage, and any provocation, hyperventilation or photic stimulation, that brought it out
- ✓Cross-check reactivity, confirm the discharge is not driven by patient stimulation or by external rhythmic input
- ✓Flag the timestamp, channel, and duration in the technologist note so the reading neurologist can navigate quickly
How clinical context changes the read
Two patients with identical waveforms can have entirely different reports. A 7-year-old with staring spells and 3 Hz spike-and-wave on hyperventilation gets a clear absence epilepsy story. A 68-year-old in the ICU with the same morphology has nonconvulsive status until proven otherwise, and the team needs to move fast. The pattern did not change. The patient did. That sounds obvious in print, but it is the thing techs forget under pressure.
Build the habit of reading the chart before you read the trace, age, medications, sedation status, last seizure, last imaging, and known antibodies. A propofol drip turns burst suppression into a goal, not a finding. A diagnosis of anti-NMDA encephalitis makes extreme delta brush expected rather than alarming. Stroke history shifts focal slowing from concerning to confirmed. The EEG is one channel of information, not the whole conversation.
Visual Reading vs Quantitative EEG
- + —
- + —
- + —
- + —
- + —
- − —
- − —
- − —
- − —
- − —
Practice habits that separate good readers from great ones
The technologists whose studies the neurologists open first share a few habits. They label clearly, they describe what they see in their own words before they reach for a label, and they document reactivity on every comatose patient without being asked. They flag artifact rather than hide it. They timestamp medication changes and clinical events on the record so the reader does not have to chase the nursing note. None of this requires extra training, just discipline.
The second habit is honest uncertainty. If you cannot tell whether a transient is a sharp wave or an electrode pop, say so. The reader can compare with adjacent epochs, ask for an impedance check, or order a recheck. A study marked as uncertain and explained is more useful than one labeled with false confidence. Boards reward this kind of reasoning too, the questions that look like trick patterns usually are not, they are clinical context tests in disguise.
Where to take this next
Pattern recognition is layered. After you have the normal awake and sleep architecture down, work systematically through the abnormal patterns one cluster at a time, focal then generalized, ictal then interictal, then the special entities like extreme delta brush and alpha coma. Pair each pattern with a clinical scenario. Reading textbook traces is fine, reading real recordings with the chart open next to you is better. Most exam questions are written by people who spent years doing exactly that.
Keep a personal pattern log. Every time you see something new on shift, save a clean epoch, write three sentences about the clinical context, and add it to the file. Six months in you will have a reference deck built from cases you actually touched, and that beats any textbook. The trace in front of you tomorrow will share more with the one you saved last Tuesday than with anything in a board review book.
One more thing worth saying out loud. The patterns in this guide do not exist to be memorized as isolated images. They exist as the visible end of a real biological process happening inside a real patient. The 3 Hz spike-and-wave is a momentary loss of thalamocortical balance. Burst suppression is cortex that has been turned almost off.
Extreme delta brush is autoimmune cortex telling you something is wrong. When you read traces that way, the patterns stop feeling like memorization and start feeling like translation. That shift is the one that turns a competent tech into the person the neurologist trusts to call them at 2 a.m.
EEG Questions and Answers
About the Author
Educational Psychologist & Academic Test Preparation Expert
Columbia University Teachers CollegeDr. Lisa Patel holds a Doctorate in Education from Columbia University Teachers College and has spent 17 years researching standardized test design and academic assessment. She has developed preparation programs for SAT, ACT, GRE, LSAT, UCAT, and numerous professional licensing exams, helping students of all backgrounds achieve their target scores.