EEG for Seizures: How the Test Diagnoses Epilepsy and What to Expect 2026 July
EEG test for seizures explained — 🆕 how it diagnoses epilepsy, how long it takes, side effects, cost, and what abnormal results actually mean.

An EEG test for seizures is the single most important diagnostic tool neurologists use when someone has had an unexplained spell, a confirmed convulsion, or a suspected episode of altered awareness. By recording the brain's electrical activity through 19 to 25 small electrodes placed on the scalp, the test can capture the abnormal discharges that define epilepsy and distinguish them from fainting, migraines, sleep disorders, or psychogenic events. For most patients, it is the first objective window into what is happening inside the brain during and between seizures.
Seizures themselves are short bursts of synchronized, excessive electrical activity in groups of neurons. Between events, many people with epilepsy still produce telltale interictal patterns — sharp waves, spikes, and spike-and-wave complexes — that an experienced reader can identify on a routine 20- to 40-minute recording. When the standard study is normal but suspicion remains high, longer recordings, sleep-deprived studies, or ambulatory EEGs increase the chance of catching the abnormality that confirms the diagnosis.
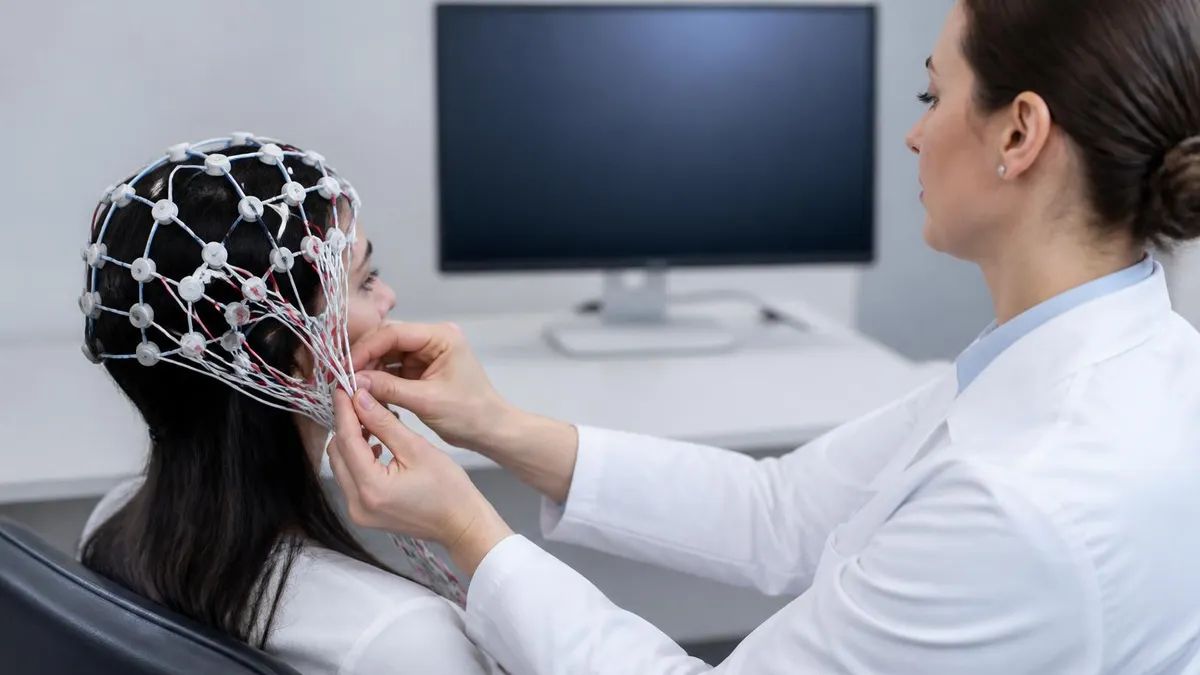
The procedure itself is painless. A trained technologist measures the head, marks specific landmarks using the international 10-20 system, and attaches electrodes with conductive paste or a stretchable cap. The signals are amplified roughly one million times and displayed as the familiar wavy traces that physicians review on screen. If you have wondered what is an eeg test actually feels like in practice, the honest answer is that it is closer to having stickers placed on your head than to any kind of imaging scan.
Patients are often surprised by how much information a non-invasive scalp recording can provide. The location of an abnormal discharge can suggest a temporal, frontal, parietal, or occipital seizure focus. The pattern — generalized 3-Hz spike-and-wave, focal sharp waves, or hypsarrhythmia — points toward specific epilepsy syndromes that respond to different medications. The presence or absence of changes during hyperventilation and photic stimulation adds further diagnostic value.
Cost is one of the most common patient questions. A routine outpatient EEG in the United States typically runs from $200 to $700 with insurance and from $700 to $3,000 without coverage, depending on the facility and whether the read is included. Long-term monitoring, inpatient video-EEG, and ambulatory studies sit in a higher range. Several keywords readers search for — eeg test price, eeg test cost, and eeg medical test fees — all point back to the same reality: prices vary widely, and asking for an itemized estimate before scheduling matters.
This guide walks through everything a patient, caregiver, or new EEG trainee needs to know about using EEG to evaluate seizures. You will learn how the test is performed, how long it takes, what abnormal findings mean, how side effects are managed, what activation procedures like flashing lights and deep breathing add to the study, and how results are translated into a treatment plan. Each section is written to be clinically accurate while still readable for someone facing their first appointment.
Whether you are preparing for a scheduled study after a single first seizure, supporting a child with absence episodes, or studying for a registry exam, the goal here is the same: to make the EEG feel less like a black box and more like a useful, understandable conversation between your brain and the neurologist reading the tracing.
EEG for Seizures by the Numbers
How the EEG Test Works
A technologist measures your head and marks 19-25 sites using the international 10-20 system. Small metal discs are attached with conductive paste or a snug cap. Placement takes about 20 minutes and is painless, though the paste can feel cool.
You lie still with eyes closed for several minutes while the machine records resting brain rhythms. The technologist will ask you to open and close your eyes, which normally suppresses the alpha rhythm — a quick check that electrodes are working correctly.
Hyperventilation for three minutes and photic stimulation with a strobe light are used to provoke abnormal activity. These maneuvers can unmask generalized spike-and-wave discharges, photoparoxysmal responses, or focal slowing that would otherwise stay hidden during a calm baseline.
Many epileptiform discharges appear only during drowsiness or stage N2 sleep. Sleep-deprived EEGs, where patients arrive after limited sleep, dramatically increase yield. The technologist may dim the room and encourage natural drowsing during the final portion of the study.
After the recording ends, a board-certified neurologist or epileptologist reviews every page, marks abnormalities, and dictates a formal report. Results are typically available within 1-5 business days and are sent to the ordering clinician for a follow-up discussion.
Understanding what an EEG looks for in seizures starts with understanding what the test actually measures. Scalp electrodes pick up the summed electrical fields produced by tens of thousands of cortical neurons firing together. When those neurons fire in their normal, slightly out-of-sync rhythm, the EEG shows the familiar background of alpha, beta, theta, and delta waves. When a population of neurons fires in tight, pathological synchrony, the waveform sharpens into spikes, sharp waves, or rhythmic discharges — the hallmarks of epilepsy.
The two broad categories every reader looks for are focal and generalized abnormalities. Focal epileptiform discharges, such as anterior temporal sharp waves, suggest a localized seizure focus that may be amenable to medication or, in select cases, surgery. Generalized discharges, such as the classic 3-Hz spike-and-wave seen in childhood absence epilepsy, point toward genetic generalized epilepsies that respond best to specific drugs like ethosuximide or valproate. The distinction shapes treatment decisions from the first office visit.
Ictal recordings — those captured during an actual seizure — are diagnostic gold. A focal seizure typically begins with rhythmic theta or alpha activity over the affected region, evolving in frequency and amplitude before spreading. A generalized tonic-clonic seizure shows generalized fast activity followed by spike-and-wave or polyspike-and-wave discharges with prominent muscle artifact. Capturing one of these on a routine study is uncommon, which is why long-term video-EEG monitoring exists.
Interictal abnormalities, recorded between seizures, are far more common and still highly informative. Sharp waves lasting 70 to 200 milliseconds, spikes shorter than 70 milliseconds, and spike-and-wave complexes all carry diagnostic weight when they appear in clinically appropriate contexts. Readers also look at the background: focal slowing in theta or delta ranges suggests underlying structural injury, while diffuse slowing points to encephalopathy or medication effects rather than pure epilepsy.
A few specific patterns deserve attention because they define syndromes. Hypsarrhythmia — chaotic, high-amplitude slowing with multifocal spikes — appears in infantile spasms. Generalized 3-Hz spike-and-wave defines childhood absence epilepsy. Centrotemporal spikes that activate in sleep characterize self-limited epilepsy with centrotemporal spikes, formerly called benign rolandic epilepsy. Each pattern carries prognostic information beyond the simple yes-or-no question of whether epilepsy is present. For a deeper reference, our page on eeg test price includes detailed pattern descriptions and reading tips.
Readers must also separate real epileptiform activity from benign variants and artifacts. Wicket spikes, 14-and-6 positive bursts, small sharp spikes of sleep, and rhythmic mid-temporal theta of drowsiness all mimic pathology but carry no clinical significance. Muscle, eye movement, sweat, and electrode pop artifacts can fool inexperienced readers. This is why formal interpretation requires board certification and ongoing case exposure rather than software alone.
Finally, a normal EEG never rules out epilepsy. Roughly half of patients with confirmed epilepsy will show a normal first routine study, and even gold-standard long-term monitoring misses occasional seizures. The diagnosis is clinical — based on the history of stereotyped events — with EEG providing critical supporting evidence. A negative result simply means abnormalities were not captured during the recording window, not that the brain is electrically normal at all times.
EEG Practice Test Questions
Prepare for the EEG - Electroencephalography exam with our free practice test modules. Each quiz covers key topics to help you pass on your first try.
EEG Abnormal Epileptiform Patterns
EEG Exam Questions covering Abnormal Epileptiform Patterns. Master EEG Test concepts for certification prep.
EEG Activation Procedures
Free EEG Practice Test featuring Activation Procedures. Improve your EEG Exam score with mock test prep.
EEG Artifact Identification
EEG Test Prep for Artifact Identification. Practice EEG Quiz questions and boost your score.
EEG Electrode Placement and Montages
EEG Questions and Answers on Electrode Placement and Montages. Free EEG practice for exam readiness.
EEG - Electroencephalography Abnormal Epil...
EEG Mock Test covering - Electroencephalography Abnormal Epileptiform Patterns. Online EEG Test practice with instant feedback.
EEG - Electroencephalography Activation Pr...
Free EEG Quiz on - Electroencephalography Activation Procedures. EEG Exam prep questions with detailed explanations.
EEG - Electroencephalography Artifact Iden...
EEG Practice Questions for - Electroencephalography Artifact Identification. Build confidence for your EEG certification exam.
EEG - Electroencephalography Electrode Pla...
EEG Test Online for - Electroencephalography Electrode Placement and Montages. Free practice with instant results and feedback.
EEG - Electroencephalography Instrumentati...
EEG Study Material on - Electroencephalography Instrumentation and Calibration. Prepare effectively with real exam-style questions.
EEG - Electroencephalography Neuroanatomy ...
Free EEG Test covering - Electroencephalography Neuroanatomy and Physiology. Practice and track your EEG exam readiness.
EEG - Electroencephalography Non-Epileptif...
EEG Exam Questions covering - Electroencephalography Non-Epileptiform Abnormalities. Master EEG Test concepts for certification prep.
EEG - Electroencephalography Normal EEG Wa...
Free EEG Practice Test featuring - Electroencephalography Normal EEG Waveforms. Improve your EEG Exam score with mock test prep.
EEG - Electroencephalography Patient Safet...
EEG Mock Exam on - Electroencephalography Patient Safety and Ethics. EEG Study Guide questions to pass on your first try.
EEG - Electroencephalography Pediatric and...
EEG Test Prep for - Electroencephalography Pediatric and Neonatal EEG. Practice EEG Quiz questions and boost your score.
EEG ICU and Continuous EEG Monitoring
EEG Questions and Answers on ICU and Continuous EEG Monitoring. Free EEG practice for exam readiness.
EEG Instrumentation and Calibration
EEG Mock Test covering Instrumentation and Calibration. Online EEG Test practice with instant feedback.
EEG Neuroanatomy and Physiology
Free EEG Quiz on Neuroanatomy and Physiology. EEG Exam prep questions with detailed explanations.
EEG Non-Epileptiform Abnormalities
EEG Practice Questions for Non-Epileptiform Abnormalities. Build confidence for your EEG certification exam.
EEG Normal EEG Waveforms
EEG Test Online for Normal EEG Waveforms. Free practice with instant results and feedback.
EEG Patient Safety and Ethics
EEG Study Material on Patient Safety and Ethics. Prepare effectively with real exam-style questions.
How Long Is an EEG Test and Which Type Do You Need
A routine outpatient EEG runs 20 to 40 minutes of actual recording, with setup and takedown bringing total appointment time to about 60 to 90 minutes. This is the standard first-line study for new-onset seizures, recurrent spells of unclear nature, or follow-up of known epilepsy on medication. It includes hyperventilation and photic stimulation in nearly every case.
The yield of a single routine study is modest — roughly 25 to 50 percent for capturing interictal epileptiform discharges in patients with confirmed epilepsy. Yield improves significantly with sleep deprivation, with repeat studies, and when the recording captures both wake and sleep stages. If your first EEG is normal but suspicion remains, expect your neurologist to recommend a longer or sleep-deprived follow-up rather than concluding the diagnosis is wrong.
EEG for Seizure Evaluation: Strengths and Limitations
- +Painless, non-invasive, and uses no radiation or contrast
- +Directly measures brain electrical activity in real time
- +Distinguishes epilepsy from syncope, migraine, and psychogenic events
- +Identifies specific epilepsy syndromes that respond to specific drugs
- +Widely available in outpatient neurology and hospital settings
- +Relatively inexpensive compared with MRI or PET imaging
- +Safe for children, pregnant patients, and those with metal implants
- −A single routine study misses about half of confirmed epilepsy cases
- −Captures interictal activity more than actual seizures
- −Cannot localize deep brain structures the way intracranial recordings can
- −Requires expert interpretation — software alone is unreliable
- −Setup with paste can be uncomfortable and leave residue in hair
- −Sleep deprivation or activation procedures may trigger seizures in vulnerable patients
- −Cost varies widely with limited transparency before scheduling
How to Prepare for Your EEG Test
- ✓Wash your hair the night before with regular shampoo only — no conditioner, oils, sprays, or gels
- ✓Skip caffeine for 8-12 hours before the test unless your physician says otherwise
- ✓Eat a normal meal beforehand — low blood sugar can alter the recording
- ✓Take all routine medications unless specifically instructed to hold seizure drugs
- ✓Bring a complete list of current medications and doses to share with the technologist
- ✓For sleep-deprived studies, stay awake the night before and arrange a ride home
- ✓Wear a comfortable shirt that buttons or zips so it does not need to go over your head
- ✓Bring a list of recent seizure events including dates, times, and descriptions
- ✓Plan to spend 60-90 minutes at the facility even for a routine study
- ✓Expect to wash hair thoroughly afterward to remove conductive paste residue
A Normal EEG Does Not Rule Out Epilepsy
Roughly 50% of patients with confirmed epilepsy show a normal first routine EEG. Diagnosis depends on clinical history plus testing — never on a single recording alone. If your study is normal but your symptoms continue, ask about a sleep-deprived or ambulatory follow-up rather than assuming epilepsy is excluded.
Cost is consistently the question patients ask first once an EEG is ordered. In the United States, a routine outpatient study generally falls between $200 and $700 when insurance covers it, with patient out-of-pocket costs ranging from a small copay to the full deductible. Without insurance, the cash price for the same study runs from roughly $700 to $3,000 depending on the facility, region, and whether the professional interpretation fee is bundled with the technical fee.
Longer studies carry proportionally higher prices. A 24- to 72-hour ambulatory EEG typically costs $1,500 to $5,000. Inpatient video-EEG monitoring in a dedicated epilepsy unit can reach $10,000 to $30,000 or more for a three- to seven-day admission, before professional fees. Patients should always request an itemized estimate that separates technical, professional, and facility components — this is the only reliable way to compare quotes between hospitals and outpatient neurology offices.
Insurance coverage is generally favorable when an EEG is ordered for a documented medical reason such as seizure evaluation, altered mental status, suspected encephalopathy, or follow-up of known epilepsy. Pre-authorization is sometimes required for ambulatory or video studies. Patients on Medicare typically pay 20 percent of the Medicare-approved amount after their deductible. Medicaid coverage varies by state but usually includes diagnostic EEG when ordered by a qualified provider.
Side effects from a standard EEG are minimal. Most patients experience nothing more than mild scalp tenderness from electrode pressure, residual paste in the hair, or a brief headache after hyperventilation. Photic stimulation can trigger a seizure in patients with photosensitive epilepsy, which is precisely why the technologist watches the recording in real time and stops the strobe at the first sign of a photoparoxysmal response. Sleep deprivation studies can leave patients drowsy, irritable, and unsafe to drive.
For patients with established epilepsy, the most discussed concern is whether the test itself might provoke a seizure. The honest answer is that it occasionally does — and that this is sometimes diagnostically useful. Technologists are trained to recognize a developing seizure, protect the patient, and document the event. The probability of a seizure during a routine outpatient study is low but real, particularly with hyperventilation or sleep deprivation in susceptible individuals.
Comparing prices between facilities is worth the effort. Outpatient neurology offices often charge less than hospital-based labs for the same routine study. Cash-pay discounts of 30 to 50 percent are common when patients ask directly. Our detailed pricing breakdown at eeg medical test walks through what each fee component actually covers and how to negotiate when a quoted price seems unreasonable. The single most useful question to ask is: "Does this price include the physician's read, or is that billed separately?"
Finally, do not let cost concerns delay a clinically necessary study. Untreated or undiagnosed epilepsy carries real risks — injury during seizures, status epilepticus, and sudden unexpected death in epilepsy (SUDEP). Most hospital systems offer financial assistance programs, payment plans, or sliding-scale fees for patients without insurance. A social worker or financial counselor at the ordering office can usually help arrange affordable access within days rather than weeks.
Patients with known photosensitive epilepsy should tell the technologist before the test begins. Photic stimulation is paused immediately if a photoparoxysmal response appears, but advance notice allows the team to use shorter flash trains and stay especially alert. Caregivers of children should likewise mention any prior reactions to flashing lights, video games, or strobes.
Receiving and interpreting EEG results is where many patients feel lost. A typical report has three parts: a clinical description of the recording, a list of findings, and a clinical impression. The description covers technical details — number of channels, montages used, length of recording, and patient state. The findings list specific abnormalities such as "left temporal sharp waves at F7-T3, occurring approximately 8 per minute during drowsiness." The impression translates those findings into clinical language: normal, abnormal due to focal epileptiform discharges, abnormal due to diffuse slowing, and so on.
The impression line is what your neurologist will discuss with you. A report reading "normal awake and drowsy EEG" means no clear abnormalities were captured during this study — it does not exclude epilepsy, as discussed earlier. "Abnormal EEG due to right temporal sharp waves" suggests a focal seizure focus consistent with temporal lobe epilepsy. "Abnormal EEG due to generalized 3-Hz spike-and-wave discharges" is essentially diagnostic of a generalized epilepsy syndrome. Each impression maps to different medication choices and follow-up plans.
Treatment decisions integrate EEG with the full clinical picture. A first unprovoked seizure with a normal EEG and normal MRI carries a roughly 30 percent two-year recurrence risk. The same first seizure with clear epileptiform discharges on EEG raises that risk to roughly 60 percent, which usually tips the decision toward starting anti-seizure medication. EEG patterns also guide drug selection — narrow-spectrum agents work well for focal epilepsy, while broad-spectrum drugs are preferred when generalized discharges are present. Our overview at what is eeg test covers how technologists and physicians collaborate on these decisions.
Follow-up timing depends on findings. A clearly abnormal study usually triggers a neurology visit within one to two weeks to start or adjust medication. A normal study with persistent symptoms often leads to a sleep-deprived repeat or an ambulatory recording within four to six weeks. Patients with controlled epilepsy on stable medication typically repeat EEGs every one to three years, or sooner if seizures break through, medications change, or withdrawal is being considered.
Special populations need tailored interpretation. In children, normal background rhythms differ markedly by age — slower posterior dominant rhythms in toddlers, prominent theta during drowsiness, and benign variants like centrotemporal spikes that may not need treatment. In older adults, diffuse slowing can reflect cerebrovascular disease, medication effects, or early neurodegeneration rather than epilepsy. In ICU patients, EEG is used to detect non-convulsive seizures, monitor sedation depth, and identify burst-suppression patterns.
For trainees and EEG technologists, the path to confident interpretation runs through deliberate practice on real tracings — recognizing benign variants, mastering the 10-20 system, and learning to separate artifact from pathology. The American Board of Registration of Electroencephalographic and Evoked Potential Technologists (ABRET) sets the standard with the R. EEG T. credential. Most clinically employed technologists complete an accredited program, log several hundred supervised recordings, and pass both written and practical examinations.
Whether you are a patient awaiting results, a parent comparing reports, or a clinician learning to read, the same principle applies: the EEG is a powerful tool, but it is one piece of a larger diagnostic puzzle. Combined with history, examination, and imaging, it provides the clarity needed to choose the right treatment and to monitor whether that treatment is working. Used well, it shortens the time from first seizure to confident diagnosis and effective care.
Practical preparation makes the EEG smoother for everyone. The night before, wash your hair with plain shampoo and skip every product that follows in a normal routine: no conditioner, no leave-in spray, no oils, no gels, no styling cream. Conductive paste needs direct contact with the scalp, and any residue acts as an insulator that lowers signal quality and lengthens setup time as the technologist scrubs each site harder than necessary.
Eat a normal meal a few hours before the appointment. Low blood sugar produces subtle slowing on the recording that can mimic mild encephalopathy and confuse interpretation. Skip caffeine for at least eight to twelve hours unless your physician specifically allows it — caffeine alters background rhythms and can suppress drowsy-stage activity that the test is trying to capture. Stay well hydrated with plain water; dehydration is another subtle confounder.
Bring a written timeline of recent events. Note dates, times, witnessed descriptions, duration, post-event confusion, tongue biting, urinary incontinence, and any triggers like sleep loss, flashing lights, or missed medication doses. This information lets the reading neurologist correlate any captured abnormalities with real-life episodes. If a family member witnessed the events, a short written account or even a phone video of a typical spell adds enormous diagnostic value.
For sleep-deprived studies, treat the preparation seriously. Stay up until your scheduled appointment, do not nap on the way, and arrange a ride to and from the facility. Driving on no sleep is genuinely dangerous and undermines the purpose of the study, because patients who arrive rested rarely reach the drowsy stages that yield the most diagnostic information. If pediatric, follow the lab's specific age-based sleep deprivation protocol rather than guessing.
After the test, give yourself time to clean up. Conductive paste washes out with warm water, a small amount of shampoo, and gentle massage — sometimes two washes are needed. Skin under electrodes may stay slightly red for an hour or two. Headaches from hyperventilation usually resolve within minutes. If you feel lightheaded or notice any unusual symptoms, tell the technologist before leaving so the team can document and address them.
Plan how you will receive results. Ask the ordering clinician's office how long interpretation typically takes — usually one to five business days — and whether results will be released through a patient portal, by phone call, or at a follow-up visit. If results show clear abnormalities, schedule the follow-up promptly so that treatment decisions are not delayed. If they are normal but your symptoms continue, push for a next step rather than accepting the result as closure.
Finally, keep your own copy. Request the formal report and, if possible, a copy of the EEG recording on a disc or through medical record release. Future neurologists, especially in second opinions or surgical evaluations, will want to compare new tracings against older ones. Patients who keep their own files generally receive faster, more coordinated care and avoid duplicate testing. The EEG is a snapshot of your brain at a single point in time — and over years of follow-up, those snapshots form the story that guides your treatment.
EEG Questions and Answers

EEG Tech Salary 2026: Pay by State, Experience, and Certification
EEG Tech Jobs in 2026: Career Paths, Salaries, and How to Get Hired

Reading EEG Patterns: A Practical Reference for Techs and Trainees

EEG Waves Explained: Delta, Theta, Alpha, Beta, and Gamma Brain Rhythms

EEG Test Cost in 2026: Prices, Insurance Coverage, and How to Save
About the Author
Educational Psychologist & Academic Test Preparation Expert
Columbia University Teachers CollegeDr. Lisa Patel holds a Doctorate in Education from Columbia University Teachers College and has spent 17 years researching standardized test design and academic assessment. She has developed preparation programs for SAT, ACT, GRE, LSAT, UCAT, and numerous professional licensing exams, helping students of all backgrounds achieve their target scores.