EEG Test Explained: What It Measures, How It Works, and How to Read the Report
EEG test terminology decoded: 📗 IED EEG meaning, eeg test price, side effects, how long an EEG takes, and how to read the report.

The EEG test is one of the most common neurological studies ordered in the United States, yet the language inside the final report can feel like a foreign dictionary. Phrases like IED, sharp wave, polyspike, photic driving, hyperventilation response, and burst suppression appear next to numbers, time stamps, and Latin abbreviations that most patients have never seen. The IED EEG meaning matters more than any other single term, because interictal epileptiform discharges are the fingerprints clinicians hunt for when a seizure is suspected but the patient is not actively convulsing in the lab.
This guide walks through EEG terminology the way a working neurodiagnostic technologist would explain it to a curious family member at the bedside. You will see plain-English translations for every common acronym, ranges for an EEG test price, expected side effects, and a tour of the report layout from the impression line down to the technical factors block. The aim is to leave you fluent enough to ask sharper questions at your next neurology follow up.
An EEG, short for electroencephalogram, records the electrical chatter of cortical neurons through small metal disks pasted to the scalp. A standard outpatient recording lasts 20 to 40 minutes, while ambulatory and inpatient studies can stretch from 24 hours to a full week. Between those bookends sit dozens of variations: routine, sleep deprived, prolonged, video EEG, long term monitoring, and quantitative EEG. Each one has its own paperwork, its own preparation rules, and its own glossary.
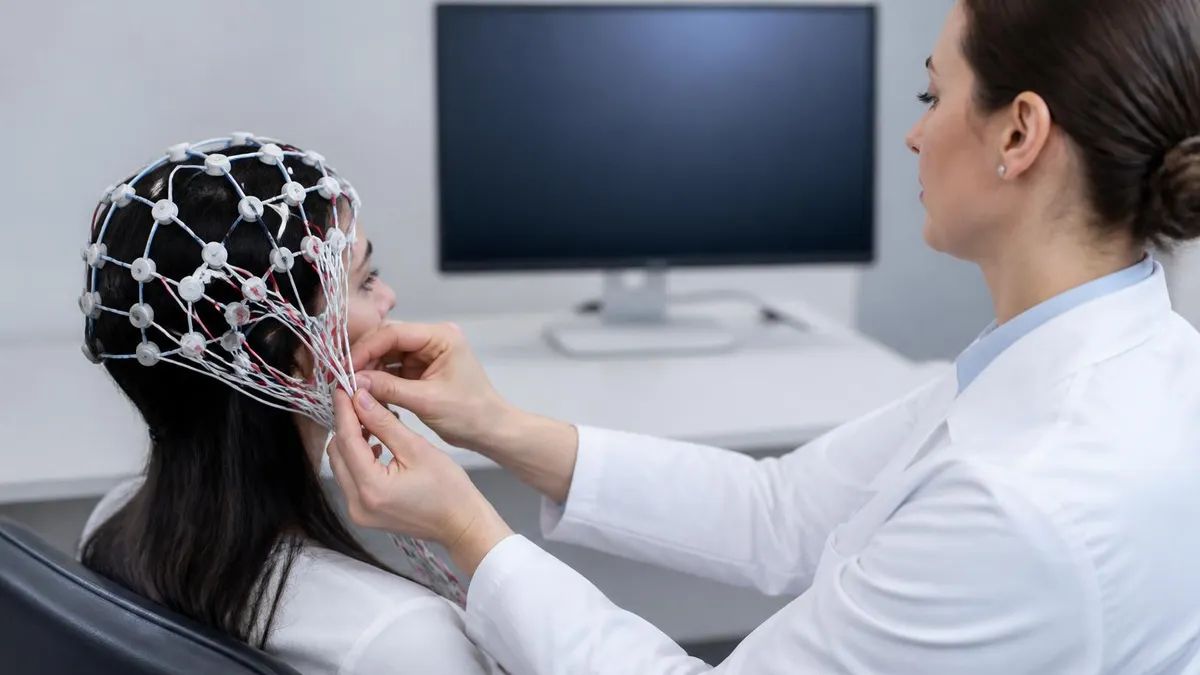
If you arrived here trying to figure out what is an eeg test in practical terms, the short version is this: it is a painless, radiation free recording that captures voltage changes on the scalp at millisecond resolution. No needles. No dye. No magnet. The technologist measures your head, marks 19 to 25 spots using the international 10 20 system, scrubs each spot with mild abrasive paste, and attaches electrodes with conductive gel or paste. The machine does the rest.
Understanding the terminology also helps you read the bill. A routine EEG test cost in the US typically lands between 200 and 1,500 dollars depending on facility, insurance contract, and whether video is included. Ambulatory studies and long term monitoring climb into the thousands. Knowing which CPT code your neurologist ordered lets you call the billing office armed with the right question rather than a vague complaint about a surprise charge.
The remainder of this article moves from foundational vocabulary to advanced report language. By the end you should be able to look at a phrase like left temporal sharp waves at F7 T3 with phase reversal at T3, occurring at 0.3 per minute during stage N2 sleep and translate it into something close to plain English. That is the level of literacy that turns a patient or a new tech trainee into a confident reader of the neurodiagnostic record.
Bookmark this page, because EEG terminology rewards repeat exposure. Each section below uses the same vocabulary in slightly different contexts so the words sink in through repetition rather than memorization. By the time you reach the FAQ you will have seen the most important terms five or six times in natural sentences, which is far more durable than any flashcard drill.
EEG Terminology by the Numbers
EEG Test Format and Setup
Technologists apply 19 to 25 cup electrodes using the international 10 20 system. Each site is named with a letter for the brain region (Fp, F, C, P, O, T) and a number for hemisphere. Odd numbers sit on the left, even numbers on the right, and z marks midline.
Before recording starts, the machine measures resistance at each electrode site. Values below 5 kilohms are ideal. High impedance creates artifact that mimics abnormalities, so the tech may re-prep skin or replace gel until every channel passes the threshold.
A 10 to 15 minute awake baseline captures resting rhythms with eyes open and closed. The tech notes drowsiness, blinks, swallows, and movement. This block establishes the patient's normal background against which any later abnormality is judged.
Hyperventilation for three minutes and photic stimulation at multiple flash frequencies are routine. These maneuvers provoke latent abnormalities that hide during quiet recording. Sleep deprivation is added when seizures are suspected but the standard study is negative.
After electrodes are removed and hair is cleaned, a board certified neurologist reads the digital file. The interpretation includes background description, abnormalities, clinical correlation, and impression. Reports typically reach the ordering provider within one to three business days.
Core EEG terminology starts with the rhythms. Delta waves run 0.5 to 4 Hz and dominate deep sleep. Theta sits at 4 to 8 Hz and shows up in drowsiness, meditation, and certain pathological states. Alpha rules the 8 to 13 Hz band and is most prominent over the posterior head when eyes are closed. Beta covers 13 to 30 Hz and reflects active concentration or medication effect. Gamma above 30 Hz is harder to capture on scalp recordings and usually requires intracranial electrodes for clean detection.
The next tier of vocabulary describes shapes. A spike lasts under 70 milliseconds and looks like a needle on the trace. A sharp wave runs 70 to 200 milliseconds and resembles a steep triangle. When a spike is followed immediately by a slow wave, the complex is called a spike and slow wave discharge. Polyspikes are runs of three or more spikes in rapid succession. These shapes matter because they form the building blocks of every epileptiform diagnosis.
IED is the abbreviation you will encounter most often if your neurologist suspects a seizure disorder. The IED EEG meaning is interictal epileptiform discharge, where interictal means between seizures, epileptiform means resembling the patterns seen in epilepsy, and discharge refers to a brief synchronized burst of neuronal firing. Finding IEDs on a routine recording strongly supports an epilepsy diagnosis even when the patient was perfectly calm during the test. Their location also guides surgical planning.
Lateralization terms describe which side of the brain a finding came from. Left, right, bilateral, generalized, focal, multifocal, and lateralized periodic discharges each carry distinct meanings. A focal finding points at one cortical region. A generalized finding involves both hemispheres simultaneously from the first millisecond. Lateralized periodic discharges, abbreviated LPDs, recur every one to two seconds and often signal acute structural injury such as stroke or encephalitis.
Frequency, amplitude, morphology, distribution, and reactivity are the five descriptors every reader applies to any waveform. Frequency answers how fast. Amplitude answers how tall, measured in microvolts. Morphology answers what shape. Distribution answers where on the head. Reactivity answers whether the pattern changes when the patient opens their eyes, hears a voice, or receives a sternal rub. Together these five tell the clinical story.
State terminology completes the foundation. Wakefulness, drowsiness, stage N1, stage N2, stage N3, and REM each have characteristic signatures. Vertex waves and sleep spindles mark N2. K complexes are large diphasic transients also seen in N2. Slow wave sleep dominates N3. REM brings low voltage mixed frequency activity with rapid eye movements visible on frontal channels. Many abnormalities only appear in specific states, which is why sleep deprivation boosts diagnostic yield. For a deeper salary perspective on the technologists who run these studies, see what is eeg test career paths.
Artifact terminology rounds out the vocabulary. Eye blink, lateral eye movement, muscle, electrode pop, sweat, ECG, pulse, 60 Hz line noise, and movement artifact each look different on the page. Recognizing artifact is half the skill of a good EEG technologist. Mistaking a chewing artifact for temporal sharp waves is one of the most common rookie errors and a major reason interpretation belongs to a trained neurologist rather than an algorithm alone.
EEG Practice Test Questions
Prepare for the EEG - Electroencephalography exam with our free practice test modules. Each quiz covers key topics to help you pass on your first try.
EEG Abnormal Epileptiform Patterns
EEG Exam Questions covering Abnormal Epileptiform Patterns. Master EEG Test concepts for certification prep.
EEG Activation Procedures
Free EEG Practice Test featuring Activation Procedures. Improve your EEG Exam score with mock test prep.
EEG Artifact Identification
EEG Test Prep for Artifact Identification. Practice EEG Quiz questions and boost your score.
EEG Electrode Placement and Montages
EEG Questions and Answers on Electrode Placement and Montages. Free EEG practice for exam readiness.
EEG - Electroencephalography Abnormal Epil...
EEG Mock Test covering - Electroencephalography Abnormal Epileptiform Patterns. Online EEG Test practice with instant feedback.
EEG - Electroencephalography Activation Pr...
Free EEG Quiz on - Electroencephalography Activation Procedures. EEG Exam prep questions with detailed explanations.
EEG - Electroencephalography Artifact Iden...
EEG Practice Questions for - Electroencephalography Artifact Identification. Build confidence for your EEG certification exam.
EEG - Electroencephalography Electrode Pla...
EEG Test Online for - Electroencephalography Electrode Placement and Montages. Free practice with instant results and feedback.
EEG - Electroencephalography Instrumentati...
EEG Study Material on - Electroencephalography Instrumentation and Calibration. Prepare effectively with real exam-style questions.
EEG - Electroencephalography Neuroanatomy ...
Free EEG Test covering - Electroencephalography Neuroanatomy and Physiology. Practice and track your EEG exam readiness.
EEG - Electroencephalography Non-Epileptif...
EEG Exam Questions covering - Electroencephalography Non-Epileptiform Abnormalities. Master EEG Test concepts for certification prep.
EEG - Electroencephalography Normal EEG Wa...
Free EEG Practice Test featuring - Electroencephalography Normal EEG Waveforms. Improve your EEG Exam score with mock test prep.
EEG - Electroencephalography Patient Safet...
EEG Mock Exam on - Electroencephalography Patient Safety and Ethics. EEG Study Guide questions to pass on your first try.
EEG - Electroencephalography Pediatric and...
EEG Test Prep for - Electroencephalography Pediatric and Neonatal EEG. Practice EEG Quiz questions and boost your score.
EEG ICU and Continuous EEG Monitoring
EEG Questions and Answers on ICU and Continuous EEG Monitoring. Free EEG practice for exam readiness.
EEG Instrumentation and Calibration
EEG Mock Test covering Instrumentation and Calibration. Online EEG Test practice with instant feedback.
EEG Neuroanatomy and Physiology
Free EEG Quiz on Neuroanatomy and Physiology. EEG Exam prep questions with detailed explanations.
EEG Non-Epileptiform Abnormalities
EEG Practice Questions for Non-Epileptiform Abnormalities. Build confidence for your EEG certification exam.
EEG Normal EEG Waveforms
EEG Test Online for Normal EEG Waveforms. Free practice with instant results and feedback.
EEG Patient Safety and Ethics
EEG Study Material on Patient Safety and Ethics. Prepare effectively with real exam-style questions.
What Is an EEG Test by Type
The routine EEG is the workhorse of outpatient neurology. It lasts 20 to 40 minutes, uses 19 to 25 electrodes, and always includes hyperventilation and photic stimulation unless contraindicated. Patients arrive with clean dry hair, no oils or conditioners, and a normal meal beforehand. The technologist measures the head, marks each site, and applies electrodes with conductive paste that washes out easily later.
Routine studies catch obvious abnormalities like generalized spike wave discharges in idiopathic generalized epilepsy or clear focal slowing over a stroke. They miss subtle findings that only appear during sleep or after a triggering event. When the clinical suspicion remains high after a negative routine EEG, the next step is usually a sleep deprived or prolonged study rather than repeating the same protocol.
Routine EEG: Strengths and Limitations
- +Painless, non-invasive, and free of radiation exposure
- +Excellent millisecond temporal resolution for electrical activity
- +Widely available at most US hospitals and many outpatient clinics
- +Affordable relative to MRI or PET for initial seizure workup
- +Repeatable as often as clinically needed without cumulative risk
- +Captures both wake and drowsy states in a single sitting
- +Provides quantitative data that algorithms can post-process
- −Limited spatial resolution compared with intracranial recording
- −Short duration may miss infrequent epileptiform discharges
- −Vulnerable to muscle, eye, and movement artifact
- −Requires patient cooperation that pediatric or agitated cases lack
- −Interpretation quality varies between readers and institutions
- −Cannot directly image brain structure or vascular anatomy
- −Sleep deprivation prep is uncomfortable for many adult patients

EEG Test Preparation Checklist
- ✓Wash hair the night before with plain shampoo only, no conditioner or styling products
- ✓Skip oils, gels, sprays, mousse, and dry shampoo on test day
- ✓Eat a normal meal before the appointment to avoid hypoglycemia artifact
- ✓Continue prescribed medications unless your neurologist gives written instructions otherwise
- ✓Bring a list of current medications and a recent seizure or spell diary
- ✓Avoid caffeine for 8 hours before a sleep deprived or routine study
- ✓Sleep no more than 4 hours the night before if a sleep deprived EEG is ordered
- ✓Wear a comfortable shirt that buttons or zips so removal does not require pulling over the head
- ✓Arrange a ride home if drowsiness or sleep deprivation is part of the protocol
- ✓Bring entertainment for any extra wait time but be ready to put it away during recording
An IED is not a seizure
The presence of interictal epileptiform discharges on an EEG does not mean the patient had a seizure during the recording. It means the brain shows a pattern statistically associated with epilepsy between events. Clinical history still drives diagnosis, and a single isolated IED in an otherwise asymptomatic adult does not automatically warrant antiseizure medication. Always correlate the report with symptoms.
EEG test price in the United States varies more widely than almost any other neurological study. A routine outpatient EEG performed at a community hospital typically bills between 200 and 800 dollars before insurance adjustments. Academic medical centers and freestanding neurodiagnostic clinics often charge 800 to 1,500 dollars for the same CPT 95812 or 95816 codes. Cash pay rates negotiated in advance can sometimes drop into the 150 to 300 dollar range, which is worth asking about if you carry a high deductible plan.
The eeg test cost equation has three layers: the technical component, the professional component, and the facility fee. The technical component covers the technologist's time, the disposable supplies, and the machine. The professional component covers the neurologist's interpretation. The facility fee covers overhead at hospital owned locations and is the single largest driver of price variation. Identical studies can cost double or triple depending on whether the facility fee applies.
Ambulatory EEG costs 1,000 to 3,000 dollars for a 24 to 72 hour recording. Long term monitoring in an epilepsy unit runs 1,500 to 4,000 dollars per day before professional fees, with typical admissions billing 10,000 to 30,000 dollars total. Insurance preauthorization is mandatory for these higher cost studies. Denials usually trace back to insufficient documentation of prior failed routine EEGs or unclear medical necessity language in the order.
Medicare and most commercial plans cover medically necessary EEGs at 80 to 100 percent after deductible. Patients on high deductible plans should call both the facility billing office and the reading neurologist's office to request itemized estimates before scheduling. The technical and professional charges often come from separate entities and arrive on separate bills weeks apart, which surprises patients who assumed one statement would cover everything.
If price is a barrier, several options exist. Hospital financial assistance programs frequently waive 50 to 100 percent of charges for patients below 300 percent of federal poverty level. Cash pay self pay rates at independent neurodiagnostic centers are often half the hospital outpatient department charge. Telehealth neurology consultations followed by EEG at an independent diagnostic testing facility can sometimes deliver a complete workup for under 600 dollars total in the right markets.
Understanding the eeg medical test billing structure also helps when interpreting an explanation of benefits. CPT 95812 covers EEGs longer than 41 minutes but under an hour. CPT 95813 covers recordings over one hour. CPT 95816 is the routine 20 to 40 minute awake and drowsy study. CPT 95819 adds a sleep component. CPT 95822 is a sleep only EEG. CPT 95957 covers digital analysis. Each code has its own reimbursement rate that you can verify against your plan's fee schedule. For technologist career details that influence facility pricing, see eeg medical test career paths.
One final cost note: the read itself is sometimes outsourced. Many community hospitals contract with regional neurology groups that read studies remotely. The professional charge appears on a separate bill from a provider you never met. This is normal and does not affect quality, but it does mean you should expect at least two statements per EEG. Confirming both ahead of time prevents the surprise that drives most patient complaints about EEG billing.
Patients with a known history of photosensitive epilepsy should inform the technologist before testing. While photic stimulation can provoke diagnostic photoparoxysmal responses, it can also trigger a generalized tonic clonic seizure in rare cases. The tech will stop the strobe immediately if epileptiform activity appears, but advance disclosure of any prior reaction to flashing lights, video games, or sun flicker is essential safety information.
EEG test side effects are minimal in the vast majority of patients, which is one reason the study is ordered so liberally. The most common complaint is a mild itchy or sticky feeling on the scalp from the conductive paste, which washes out completely with one or two regular shampoos. Some patients notice small red marks at electrode sites for a day or two, particularly when the tech needed extra abrasive prep to lower impedance on a few stubborn channels. None of these effects require treatment.
Hyperventilation for three minutes can produce transient lightheadedness, tingling in the fingers and around the mouth, and a feeling of being slightly out of breath. These symptoms resolve within a minute of returning to normal breathing. Patients with a history of stroke, sickle cell disease, severe asthma, or recent cardiac events should mention these conditions because hyperventilation is contraindicated or modified in those cases. The technologist will defer the maneuver based on the screening questions.
Photic stimulation rarely causes problems for non photosensitive patients. A small percentage of people experience mild headache or eye strain after the strobe. Patients with photosensitive epilepsy are at theoretical risk for a triggered seizure, although protocols stop the flash immediately at the first sign of photoparoxysmal response. Pregnancy is not a contraindication for any standard EEG component, and the test exposes the fetus to no radiation or chemical risk whatsoever.
Sleep deprivation protocols carry their own minor risks. Driving home after a sleep deprived EEG is discouraged because reaction time and judgment are measurably impaired. A friend, family member, or rideshare is the standard recommendation. Patients with bipolar disorder or a history of mania triggered by sleep loss should discuss the protocol with their psychiatrist before scheduling, since acute sleep deprivation can sometimes precipitate a mood episode.
For long term monitoring patients, skin breakdown under electrodes is the most realistic adverse effect. Modern collodion based attachments rarely cause damage during a three to seven day admission, but pressure injuries can develop in immobile or comatose patients. EEG technologists rotate or refresh electrodes on schedule and document any skin findings during each shift. Family members can ask to see the skin check notes if they have concerns about pressure areas.
Allergic reactions to electrode paste, gel, or collodion adhesive occur in well under one percent of patients. Symptoms include localized redness, itching, or a small rash that resolves within days of removal. Patients with known sensitivity to medical adhesives should mention this in advance so the team can substitute a hypoallergenic alternative. For deeper pattern recognition training that helps techs avoid prolonged electrode contact issues, review eeg test price related guidance.
The bottom line on safety is reassuring. An EEG is among the lowest risk diagnostic procedures in modern medicine. The benefits of accurate seizure characterization, sleep staging, encephalopathy detection, and brain death evaluation vastly outweigh the small inconveniences of paste in the hair and a few minutes of fast breathing. Decades of clinical experience confirm that even repeated EEGs across a lifetime carry no cumulative harm of any kind.
Practical tips for reading your own EEG report start with the impression line. Neurologists place the most clinically actionable summary in the impression, usually one to three sentences at the bottom of the page. Phrases like normal awake and drowsy EEG, abnormal due to left temporal sharp waves, or abnormal due to generalized spike and slow wave discharges tell you the headline finding. Everything above the impression is supporting documentation for that final statement.
Look next at the technical factors block. This tells you what was actually recorded: duration, electrode placement, sampling rate, filter settings, and whether activation procedures were performed. If hyperventilation or photic stimulation was deferred, the reason will appear here. A study without activation has lower diagnostic sensitivity, which matters when interpreting a negative result in a patient with strong clinical suspicion of seizures.
The background section describes baseline rhythms. A normal adult awake background shows a well organized posterior dominant rhythm of 8.5 to 12 Hz that attenuates with eye opening. Abnormal backgrounds include diffuse slowing, focal slowing, asymmetry, or absence of the expected posterior rhythm. Each of these has differential diagnoses ranging from medication effect to structural lesion to encephalopathy, which the neurologist correlates with clinical history.
Sleep architecture appears in its own paragraph when sleep was captured. Look for mentions of stage N1, N2, N3, and REM. Vertex waves, sleep spindles, K complexes, and slow wave sleep should be noted by stage. Absence of expected sleep features in a study that lasted long enough to capture them is itself a finding. So is the presence of sleep activated epileptiform discharges that did not appear during wakefulness.
Abnormalities are described by frequency, amplitude, morphology, location, and frequency of occurrence. A report might read sharp waves of moderate amplitude maximal at F7 and T3 with phase reversal at T3, occurring at approximately 0.5 per minute during stage N2 sleep. Translated, this means epileptiform sharp waves over the left anterior temporal region, of clinically meaningful but not extreme size, occurring once every two minutes during light sleep, with the electrical source localized just under the T3 electrode.
Compare current findings to any prior EEG report your neurologist references. Stability, improvement, or worsening of a known abnormality is often more clinically meaningful than the absolute description on a single study. A patient whose IED burden dropped from 12 per hour to 1 per hour after medication adjustment is responding well, even if both reports use the word abnormal. Trends matter as much as snapshots in EEG interpretation.
Finally, do not hesitate to ask questions at your follow up visit. Bring the report, a highlighter, and a list of terms that did not make sense. Most neurologists welcome informed patients because the conversation moves faster and treatment decisions land on firmer shared ground. EEG literacy is not gatekept, and the vocabulary you learned in this article is the same vocabulary used at the bedside, in residency conferences, and in published epilepsy research.
EEG Questions and Answers

EEG for Seizures: How the Test Diagnoses Epilepsy and What to Expect

EEG Tech Salary 2026: Pay by State, Experience, and Certification
EEG Tech Jobs in 2026: Career Paths, Salaries, and How to Get Hired

Reading EEG Patterns: A Practical Reference for Techs and Trainees

EEG Waves Explained: Delta, Theta, Alpha, Beta, and Gamma Brain Rhythms
About the Author
Educational Psychologist & Academic Test Preparation Expert
Columbia University Teachers CollegeDr. Lisa Patel holds a Doctorate in Education from Columbia University Teachers College and has spent 17 years researching standardized test design and academic assessment. She has developed preparation programs for SAT, ACT, GRE, LSAT, UCAT, and numerous professional licensing exams, helping students of all backgrounds achieve their target scores.