Trump and MRI: What Presidential Health Scans Reveal About Modern Magnetic Resonance Imaging
Trump and MRI scans explained: what presidential health exams reveal about modern MRI technology, protocols, and what radiologists look for. 🎯

The intersection of trump and mri has captured public attention every time a sitting or former U.S. president undergoes a medical examination. When high-profile individuals submit to MRI scanning, it shines a spotlight on what this powerful imaging technology can and cannot detect, how results are interpreted by board-certified radiologists, and why the general public benefits from understanding the basics of magnetic resonance imaging protocols. Presidential health disclosures, however partial, have repeatedly sparked national conversations about neurological wellness, cardiovascular risk, and cognitive function — all areas where MRI plays a central diagnostic role.
Magnetic resonance imaging uses powerful magnetic fields and radiofrequency pulses to generate extraordinarily detailed cross-sectional images of the body's internal structures without exposing patients to ionizing radiation. Unlike X-rays or CT scans, MRI excels at differentiating soft tissue — making it the preferred modality for evaluating the brain, spinal cord, joints, and abdominal organs. When physicians order an MRI for any patient, including a head of state, they are seeking information that plain films and blood tests simply cannot provide. Understanding those distinctions helps the public contextualize health bulletins issued by the White House physician's office.
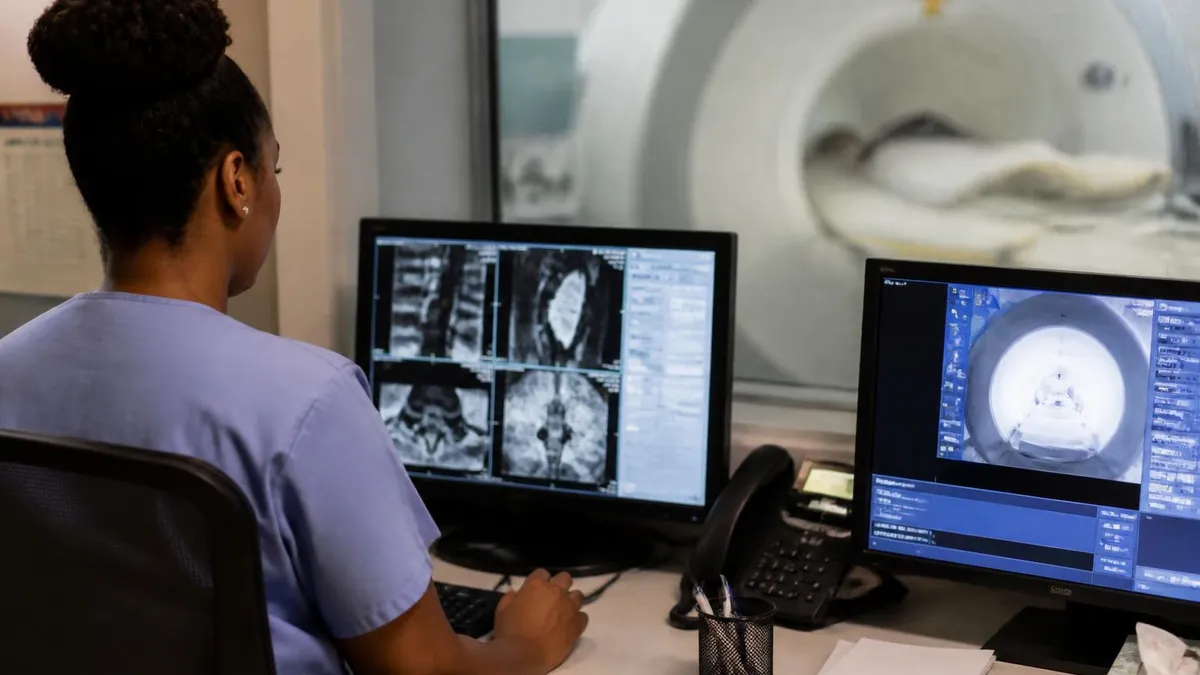
Donald Trump's annual physicals at Walter Reed National Military Medical Center have included neurological assessments that prompted widespread media discussion about what specific tests were — and were not — performed. In 2018, then-President Trump underwent a Montreal Cognitive Assessment, a brief bedside screening tool, but questions persisted about whether a full brain MRI had been ordered. The distinction matters enormously to radiologists and neurologists: a cognitive screening pencil-and-paper test measures observable behavior, whereas an MRI reveals structural anatomy, white matter integrity, and vascular changes invisible to behavioral observation.
Brain MRI protocols ordered for patients with cognitive concerns typically include T1-weighted sequences for anatomical detail, T2-weighted and FLAIR sequences to detect white matter hyperintensities and demyelinating lesions, and diffusion-weighted imaging to identify acute or subacute ischemic changes. For a deeper look at how diffusion techniques work, the trump mri resource on diffusion-weighted imaging provides a comprehensive technical overview of the sequences most relevant to neurological evaluation. Each sequence answers a different clinical question, and a complete neurological MRI workup may require 45 to 75 minutes in the scanner.
Presidential health transparency has evolved considerably over the past century. Franklin Roosevelt's polio-related paralysis was largely hidden from the public, while John F. Kennedy's Addison's disease and chronic back pain were managed in near-total secrecy. Today, release of a sitting president's annual physical — including select imaging results — is considered a baseline expectation by most journalists, medical ethicists, and the public. When those disclosures are incomplete or ambiguous, radiologists and physicians frequently explain to the media what a thorough MRI workup would entail, effectively educating millions about imaging medicine.
The neurological question looms largest in discussions of presidential MRI. Age-related changes visible on brain MRI include cortical atrophy, periventricular white matter changes, lacunar infarcts, and microhemorrhages — findings that may or may not correlate with measurable cognitive decline depending on their location, extent, and trajectory over serial examinations. A single normal MRI cannot rule out early neurodegenerative disease; conversely, incidental findings on a first-time scan may alarm patients and families without indicating any functional impairment. Radiologists spend years learning to contextualize findings within clinical history.
For MRI technologists, radiographers, and students preparing for board certification, the public discourse around high-profile MRI exams creates a unique teaching moment. Understanding which sequences detect which pathologies, why contrast agents are or are not administered, and how radiologists communicate findings in their reports are all foundational competencies. The broader conversation about what presidential health disclosures do and do not reveal maps neatly onto the curriculum covered in MRI board exams — from physics and instrumentation to anatomy, pathology, and patient safety protocols.
Presidential Health and MRI by the Numbers
What a Presidential Brain MRI Actually Evaluates
T1-weighted sequences map gray and white matter volumes, ventricular size, and cortical thickness. Volumetric analysis can detect atrophy patterns consistent with specific neurodegenerative conditions long before symptoms become functionally limiting.
T2-FLAIR sequences highlight hyperintensities in periventricular and subcortical white matter. These findings correlate with vascular risk factors, hypertension, and age, and their location guides clinical interpretation significantly.
Gradient echo and susceptibility-weighted imaging detect microhemorrhages and hemosiderin deposits. Lacunar infarcts appear as small focal T2 signal abnormalities and indicate prior small-vessel ischemic events.
Diffusion-weighted imaging identifies acute ischemia within minutes of onset. Perfusion MRI maps cerebral blood flow and can reveal tissue at risk, guiding treatment decisions in acute stroke scenarios.
Resting-state fMRI and DTI tractography reveal how different brain regions communicate. These advanced sequences are used in research and select clinical contexts to map neural networks affected by age or disease.
Understanding MRI protocols begins with appreciating that no single sequence provides all the clinical information a radiologist needs. Each pulse sequence is designed to emphasize different tissue properties — specifically the longitudinal relaxation time T1, the transverse relaxation time T2, and the diffusion of water molecules. A standard brain MRI ordered by a neurologist will typically include at minimum a sagittal T1, axial T2, axial FLAIR, axial diffusion-weighted imaging with ADC maps, and axial gradient echo sequences. More specialized clinical questions prompt additional sequences, including MR angiography, spectroscopy, or perfusion imaging.
T1-weighted images are the anatomical workhorse of brain MRI. On T1, fat and subacute blood appear bright (hyperintense), while water and cerebrospinal fluid appear dark (hypointense). Gray matter is slightly darker than white matter on standard T1 images, which allows radiologists to assess cortical ribbon thickness, identify focal lesions, and evaluate post-contrast enhancement when gadolinium-based contrast is administered. Gadolinium shortens T1 relaxation time in vascularized or inflamed tissue, causing those regions to appear bright relative to background brain parenchyma.
T2-weighted and FLAIR sequences are the primary tools for detecting pathology in the brain parenchyma. On T2 images, water appears bright, which means edema, demyelination, gliosis, and many tumors stand out clearly against darker surrounding tissue. FLAIR — Fluid Attenuated Inversion Recovery — suppresses the normally bright CSF signal so that periventricular lesions immediately adjacent to the ventricles remain visible rather than being obscured by high signal from the surrounding CSF. This distinction is clinically critical for conditions like multiple sclerosis, where periventricular plaques are a diagnostic hallmark.
Diffusion-weighted imaging revolutionized acute stroke care by enabling detection of cytotoxic edema — the hallmark of acute ischemia — within minutes of onset, far earlier than T2 signal changes appear. DWI measures the random Brownian motion of water molecules within tissue compartments. In healthy brain tissue, water diffuses freely; in acutely ischemic brain tissue, cell swelling restricts diffusion, producing high signal on DWI and low apparent diffusion coefficient values on ADC maps. This combination of findings is considered highly specific for acute infarction and guides emergency treatment decisions including IV thrombolysis and mechanical thrombectomy.
Susceptibility-weighted imaging and gradient echo sequences detect blood products and calcifications by exploiting the magnetic susceptibility differences between these materials and surrounding tissue. Microhemorrhages appear as small round hypointense foci, often scattered throughout the brain in conditions like cerebral amyloid angiopathy or chronic hypertensive small-vessel disease. The presence and distribution pattern of microhemorrhages has important implications for anticoagulation decisions and represents a finding that would never appear on a standard clinical cognitive assessment — illustrating exactly why paper-and-pencil tests and MRI answer fundamentally different clinical questions.
MR angiography allows non-invasive visualization of the intracranial and cervical vasculature. Time-of-flight MRA exploits the inflow of unsaturated blood into the imaging plane to generate vessel contrast without any contrast injection, while contrast-enhanced MRA provides higher spatial resolution and better visualization of smaller vessels. For patients with suspected arterial stenosis, aneurysm, or arteriovenous malformation, MRA is an essential component of the imaging workup. In presidential health contexts, carotid artery stenosis and intracranial aneurysm would both be relevant clinical concerns in older male patients with vascular risk factors.
Contrast administration with gadolinium-based agents raises patient safety questions that every MRI technologist must understand thoroughly. Gadolinium can accumulate in the brain, particularly the dentate nucleus and globus pallidus, even in patients with normal renal function, though the clinical significance of this deposition remains an active area of research. In patients with severe renal impairment, gadolinium carries a risk of nephrogenic systemic fibrosis, a potentially serious fibrotic condition. These safety considerations inform the decision-making process every time a radiologist considers whether contrast will meaningfully change clinical management — a cost-benefit analysis applied to every patient regardless of their public profile.
How Radiologists Interpret Neurological MRI Findings
Distinguishing normal age-related brain changes from pathological findings is one of the most nuanced skills in neuroradiology. Mild cortical atrophy, small periventricular white matter hyperintensities, and prominent perivascular spaces are all commonly seen in healthy adults over age 60 and do not in isolation indicate disease. Radiologists evaluate the degree, distribution, and progression of these changes in the context of the patient's age, vascular risk profile, and clinical presentation before assigning diagnostic significance.
When findings exceed expected age-related changes — for instance, asymmetric hippocampal volume loss, extensive confluent white matter disease, or cortical diffusion restriction — the report will flag these as clinically significant. Serial imaging, comparing current scans to prior studies, is often the most powerful tool for distinguishing stable incidental findings from progressing pathology. This is why maintaining a longitudinal imaging record matters enormously, and why a single normal MRI cannot definitively exclude early neurodegeneration.

MRI for Neurological Assessment: Strengths and Limitations
- +No ionizing radiation, making serial imaging safe for long-term monitoring
- +Superior soft tissue contrast compared to CT, X-ray, or ultrasound
- +Multiple sequences answer different clinical questions in a single exam session
- +Can detect acute ischemic stroke within minutes using diffusion-weighted imaging
- +Non-invasive vascular imaging possible without catheter-based angiography
- +Functional and metabolic information available through advanced sequences like fMRI and spectroscopy
- −Longer scan times (45–75 minutes) compared to CT (minutes), limiting use in unstable patients
- −Contraindicated for patients with certain metallic implants, pacemakers, or cochlear implants
- −Claustrophobia affects a significant minority of patients, sometimes requiring sedation
- −Higher cost than CT, often $1,000–$5,000 depending on body part and facility
- −Motion artifacts degrade image quality, especially in uncooperative or agitated patients
- −Gadolinium contrast carries renal and potential deposition risks that require careful patient selection
Pre-Scan Checklist: What Every Brain MRI Patient Should Do
- ✓Inform your ordering physician and MRI technologist of all metallic implants, including dental work, surgical hardware, and embedded devices.
- ✓Disclose any prior allergic reactions to contrast agents or iodine-based dyes before your appointment.
- ✓Bring a complete list of current medications, as some can affect renal function relevant to gadolinium safety screening.
- ✓Remove all ferromagnetic jewelry, piercings, and hair accessories before entering the MRI suite.
- ✓Wear comfortable, metal-free clothing or change into a hospital gown provided by the facility.
- ✓Arrive 15–30 minutes early to complete safety screening paperwork and answer the MRI safety questionnaire thoroughly.
- ✓Inform staff if you experience claustrophobia so that open MRI options, mirror glasses, or anxiolytic medication can be arranged in advance.
- ✓Arrange transportation if sedation or anesthesia has been planned, as you will not be able to drive afterward.
- ✓Ask your physician whether contrast will be used and whether your renal function has been checked if you have kidney disease or diabetes.
- ✓Fast for 4–6 hours before the scan if contrast or sedation is planned, unless instructed otherwise by your physician.
One Normal MRI Does Not Rule Out Neurodegeneration
A single brain MRI showing no acute abnormality is reassuring but cannot exclude early neurodegenerative disease. Conditions like Alzheimer's disease may show minimal or no structural changes on MRI in their earliest clinical stages. Serial imaging over time — comparing scans 12 to 24 months apart — is far more informative than any single snapshot, which is why ongoing longitudinal monitoring matters for all patients, including those at high public visibility.
When evaluating the full picture of presidential health, it is essential to place MRI within the broader landscape of diagnostic tools available to the White House medical team. Annual physicals for U.S. presidents typically include a comprehensive physical examination, complete blood count, comprehensive metabolic panel, lipid profile, thyroid function tests, cardiac stress testing, and pulmonary function assessment. Each modality answers different questions: blood tests reveal systemic biochemical status, stress testing evaluates cardiac reserve under physiological load, and MRI provides structural anatomical detail of specific organ systems. No single test captures the whole patient.
CT scanning is often ordered alongside or instead of MRI in acute or emergency settings because of its speed and wider availability. A non-contrast CT of the head can rule out large hemorrhage, major mass effect, or significant hydrocephalus within minutes. However, CT uses ionizing radiation and provides far less soft tissue contrast than MRI, making it a complementary rather than equivalent tool. In the context of a scheduled annual physical for a stable, ambulatory patient, MRI is the preferred modality for neurological evaluation when clinical concerns justify the examination.
Cardiac MRI, though less discussed in media coverage of presidential health, represents another powerful application of the technology. Cardiac MRI can precisely quantify left ventricular ejection fraction, assess myocardial viability, identify infiltrative cardiomyopathies, and evaluate pericardial disease — all with a level of accuracy that exceeds echocardiography in many clinical scenarios. For older male patients with cardiovascular risk factors, cardiac MRI would provide clinically meaningful information beyond what standard stress testing and echocardiography can offer. Its limited use in routine executive physicals reflects pragmatic considerations about time, cost, and clinical indication rather than any technological limitation.
Whole-body MRI screening protocols have gained interest in concierge medicine and executive health programs as a tool for detecting early occult malignancy and vascular disease in asymptomatic high-risk individuals. These protocols typically scan the brain, cervical and thoracic spine, chest, abdomen, and pelvis in a single extended session lasting two to three hours.
While comprehensive, whole-body MRI screening generates substantial incidental findings — anatomical variants and benign lesions that require further workup, cause patient anxiety, and drive additional healthcare utilization without clear mortality benefit in unselected populations. Radiological and medical societies have not endorsed whole-body MRI as a routine screening tool outside of specific high-risk hereditary cancer syndromes.
Nuclear medicine imaging, including PET scanning with amyloid tracers such as florbetapir and flortaucipir, represents the current frontier for diagnosing Alzheimer's disease in living patients. Amyloid PET detects fibrillar amyloid plaques in the brain with high sensitivity and specificity, providing diagnostic information that structural MRI cannot — MRI can show the downstream consequences of neurodegeneration (atrophy, white matter changes) but cannot directly visualize the protein aggregates driving pathological processes.
FDA approval of lecanemab and donanemab, two amyloid-targeting immunotherapies, has made amyloid PET or CSF biomarker confirmation a clinical necessity before initiating treatment, raising the stakes for accurate early diagnosis in all patients, not just public figures.
The ethical dimensions of public health disclosure intersect with genuine clinical complexity in ways that require medical literacy to navigate. When a White House physician states that a president is fit for duty, that statement reflects a clinical judgment that depends on the specific duties being assessed, the standards applied, and the information available at the time of examination.
Radiological findings exist on a spectrum: a report of no acute intracranial abnormality is meaningfully different from a report of no intracranial abnormality, which is itself different from a comprehensive statement about age-appropriate versus age-inappropriate findings. Educating the public about these distinctions is part of the broader social role that medical professionals and science communicators play in democratic societies.
For MRI students and technologists preparing for registry examinations, the public conversation about presidential health has an unexpected educational upside: it provides real-world clinical context for concepts typically encountered only in textbooks. When a news anchor asks whether a cognitive screening test is equivalent to a brain MRI, the correct answer — no, they measure entirely different things — encapsulates a foundational concept in diagnostic medicine.
When media reports describe a scan as showing white matter changes, students can apply their knowledge of T2-FLAIR sequences, vascular risk factors, and clinical correlation to understand what that finding does and does not mean. The best MRI professionals are not only technically skilled but also capable of translating complex imaging concepts for patients and the public with clarity and precision.

Information released in presidential health summaries represents a curated subset of the complete medical record. Radiological reports may contain incidental findings, technical notes, and clinical context that are not included in public briefings. Readers should interpret disclosed results accordingly, understanding that absence of mentioned findings does not equal absence of all findings — and that selective disclosure is standard practice in both clinical and public health contexts.
For MRI technologists and students, mastering the technical foundations of MRI is inseparable from understanding the clinical context in which those scans are ordered and interpreted. The physics of magnetic resonance — from the behavior of hydrogen protons in a static magnetic field to the mechanics of radiofrequency excitation and signal detection — underpins every image quality decision made in the scanner room. Technologists who understand why specific pulse sequence parameters produce specific tissue contrasts are far better equipped to troubleshoot artifacts, optimize protocols, and adapt to clinical scenarios that fall outside standard operating procedures.
Magnetic field strength is one of the most consequential variables in MRI image quality. Clinical scanners range from 0.3 Tesla open systems used for claustrophobic or bariatric patients to 3 Tesla systems standard at major academic medical centers and now 7 Tesla ultra-high-field systems entering clinical use for specialized neurological applications. Higher field strength improves signal-to-noise ratio, enabling thinner slices, smaller voxels, and shorter scan times — but also increases susceptibility artifacts, chemical shift effects, and radiofrequency energy deposition (SAR). Technologists must understand these tradeoffs to make informed decisions when adapting protocols to individual patients and clinical questions.
Gradient systems are responsible for spatial encoding — the process by which the MRI system assigns spatial location to each signal it receives. The gradient amplitude (measured in mT/m) and slew rate (measured in T/m/s) determine how quickly and precisely the system can switch gradients, directly affecting echo times, repetition times, and the speed at which specific sequences can be executed.
High-performance gradient systems enable advanced techniques including echo planar imaging for DWI and fMRI, reducing acquisition times dramatically. Peripheral nerve stimulation from rapidly switching gradients represents a regulatory safety constraint that limits how aggressively gradient performance can be pushed in clinical practice.
Radiofrequency coils serve as both transmitters of RF energy and receivers of the faint MRI signal emanating from the patient. Phased-array receiver coils, composed of multiple small coil elements arranged strategically around the anatomy of interest, provide superior signal-to-noise ratio compared to single-element coils by placing sensitive receivers in close proximity to the signal source. Parallel imaging techniques like GRAPPA and SENSE exploit the spatial information encoded in phased-array coil elements to accelerate data acquisition by undersampling k-space and using coil geometry to recover missing information, reducing scan time by factors of two to four without proportionally degrading image quality.
K-space is the raw data domain in which MRI data is collected before Fourier transformation converts it into the familiar anatomical images displayed on reading workstations. The center of k-space determines image contrast, while the periphery encodes fine spatial detail. Understanding k-space geometry explains why certain artifacts — ghosting, ringing, truncation — appear where they do and how acquisition strategies can be modified to reduce their impact. For registry exam candidates, k-space concepts are reliably tested and represent an area where conceptual clarity distinguishes top performers from those who have only memorized surface facts.
MRI safety encompasses three primary hazard categories: projectile effects from ferromagnetic objects drawn into the magnetic field, thermal injury from RF energy deposition in electrically conductive implants or tissue, and acoustic noise from gradient switching that can cause temporary or permanent hearing damage.
The static magnetic field presents the most dramatic and instantaneous safety risk — a ferromagnetic oxygen tank or floor buffer becomes a potentially lethal projectile in seconds within a high-field MRI environment. The four-zone safety model developed by the American College of Radiology provides the structural framework for designing MRI facilities that prevent unauthorized access and control ferromagnetic hazards systematically.
Registry preparation for the ARRT MRI examination requires command of all these technical domains alongside patient care, anatomy, pathology, and image production. Candidates who approach the examination with deep conceptual understanding rather than surface memorization consistently outperform those who rely on mnemonics alone. Practice examinations that mirror the registry format — including physics questions on relaxation times, safety questions on implant screening, and anatomy questions on cross-sectional neurological imaging — are among the most effective preparation tools available to candidates in the final weeks before their examination date.
Preparing effectively for the ARRT MRI registry examination requires a structured approach that builds conceptual understanding progressively over weeks, not days. The most successful candidates begin their preparation at least 12 to 16 weeks before their examination date, using the early weeks to reinforce foundational physics concepts before advancing to clinical applications, anatomy, and pathology. Attempting practice questions before understanding the underlying physics concepts produces shallow pattern-matching rather than transferable knowledge — a distinction that becomes apparent when the exam presents questions in unfamiliar formats or clinical contexts.
Physics review should begin with the fundamental behavior of hydrogen protons in static magnetic fields: the concept of precession, the Larmor equation relating precession frequency to field strength, longitudinal and transverse magnetization, and the mechanisms of T1 and T2 relaxation.
From this foundation, candidates can build understanding of pulse sequences — how varying TR and TE produces different tissue contrasts, why short TR and short TE produces T1 weighting, and why long TR and long TE produces T2 weighting. These relationships are not arbitrary conventions to memorize but logical consequences of the underlying physics, and understanding the logic makes examination questions far more tractable.
Anatomy review for the MRI registry should focus on cross-sectional appearance in all three standard planes — axial, coronal, and sagittal — for the major body regions covered by the examination: brain, spine, musculoskeletal system, abdomen, and pelvis. Brain anatomy in particular requires detailed knowledge of cortical gyri and sulci, deep gray matter structures including the basal ganglia and thalamus, white matter tracts, the ventricular system, and posterior fossa structures including the cerebellum, pons, medulla, and cranial nerve exit points. Each structure has a characteristic signal intensity on T1, T2, and FLAIR that experienced technologists recognize instantly.
Pathology questions on the MRI registry examine candidates' ability to recognize characteristic imaging appearances of common conditions: cerebral infarction, multiple sclerosis plaques, meningioma, glioblastoma, herniated disc, rotator cuff tear, meniscal injury, liver hemangioma, renal cell carcinoma, and uterine fibroid, among others. Each condition has specific features — location, signal characteristics, enhancement pattern, mass effect, and associated findings — that distinguish it from mimics. Systematic review of these conditions using annotated case-based materials is more effective than reading descriptive text alone, because visual pattern recognition is the actual cognitive skill being tested.
Patient care competencies tested on the registry examination include contrast agent safety screening, monitoring of sedated patients, management of claustrophobia, recognition of contrast reactions, and appropriate response to medical emergencies in and around the MRI environment. Technologists must know which vital sign changes warrant immediate intervention, when to call for emergency assistance, and how to safely remove patients from the MRI scanner without introducing ferromagnetic hazards. These competencies are not merely examination topics but real-world skills that protect patient safety in clinical practice.
Time management during the registry examination itself is a skill that benefits from deliberate practice. The ARRT MRI examination consists of 200 questions administered over three hours, allowing an average of 54 seconds per question. Most candidates find that the majority of questions can be answered confidently in 20 to 30 seconds, leaving additional time for the minority of questions that require careful analysis or elimination of incorrect options.
Developing comfort with pacing — answering quickly on high-confidence items and budgeting extra time for complex physics calculations or nuanced clinical scenarios — comes from repeated exposure to timed practice examinations under simulated testing conditions.
Community and accountability significantly enhance examination preparation outcomes. Study groups, online forums, and structured review courses provide both social accountability and exposure to the questions and explanations of other candidates who may approach material from different angles. When one candidate's explanation of a concept illuminates what a textbook description left opaque, both candidates benefit. The best examination preparation combines independent review of core content, active recall through practice questions, peer discussion to consolidate understanding, and systematic tracking of performance across content domains to identify and address persistent weak areas before examination day.
MRI Questions and Answers

DWI MRI: Diffusion-Weighted Imaging Explained (2026 Guide)
Side Effects of Brain MRI: Understanding Risks, Safety, and What Every Patient Should Know
MRI Lumbar Spine Without Contrast: Complete Guide to the Scan, What It Shows, and How to Prepare

MRI History: From Nuclear Resonance to Modern Scanners

MRI of Cervical Spine: Complete Guide to Imaging, Anatomy, Pathology, and Patient Preparation
About the Author
Medical Laboratory Scientist & Clinical Certification Expert
Johns Hopkins UniversityDr. Sandra Kim holds a PhD in Clinical Laboratory Science from Johns Hopkins University and is certified as a Medical Technologist (MT) and Medical Laboratory Scientist (MLS) through ASCP. With 16 years of clinical laboratory experience spanning hematology, microbiology, and molecular diagnostics, she prepares candidates for ASCP board exams, MLT, MLS, and specialist certification tests.
Join the Discussion
Connect with other students preparing for this exam. Share tips, ask questions, and get advice from people who have been there.
View discussion (4 replies)