Normal MRI Brain: What a Healthy Scan Looks Like and How to Interpret Results
Learn what a normal MRI brain scan looks like, how radiologists interpret results, 🆕 key anatomy landmarks, and what findings mean for patients.

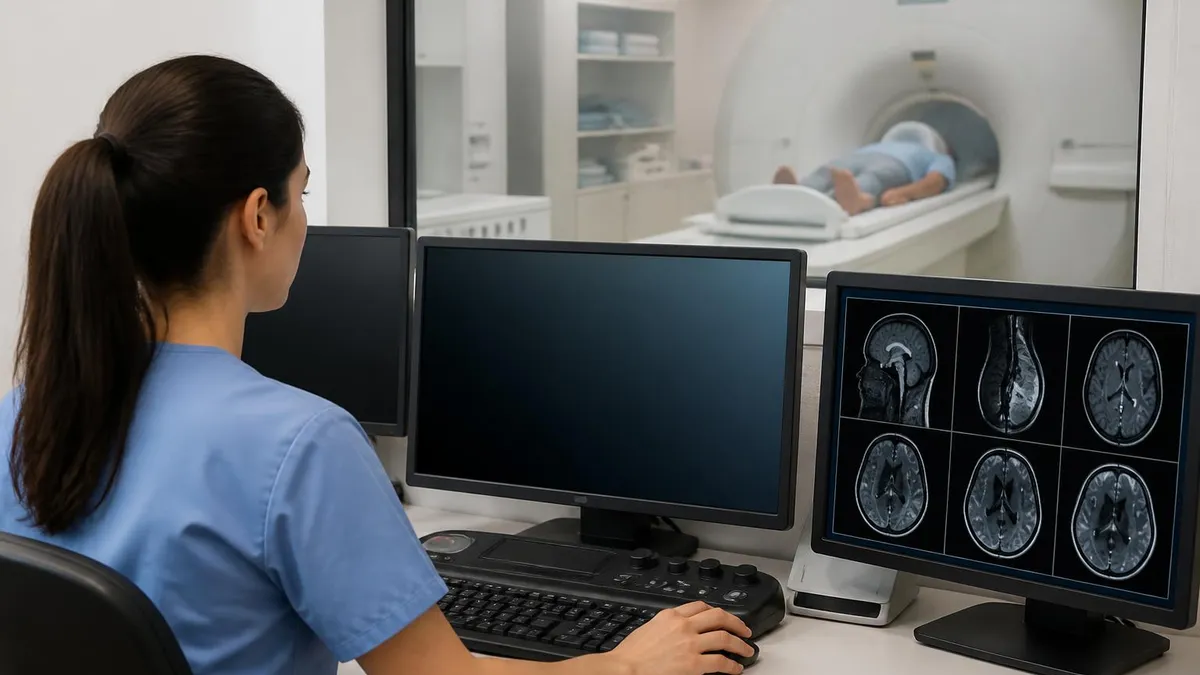
A normal MRI brain scan is one of the most reassuring findings a patient can receive after undergoing neurological imaging. Understanding what a healthy brain looks like on magnetic resonance imaging helps patients interpret their reports with confidence and allows student technologists to build the foundational knowledge needed for certification exams. When radiologists describe a normal MRI brain, they are confirming that the brain's gray matter, white matter, ventricles, sulci, gyri, and vascular structures all appear within expected parameters for the patient's age and clinical history.
Brain MRI has become the gold standard for neurological evaluation because it provides unparalleled soft tissue contrast without exposing patients to ionizing radiation. A standard brain MRI protocol typically includes T1-weighted, T2-weighted, FLAIR (Fluid-Attenuated Inversion Recovery), and diffusion-weighted sequences. Each sequence highlights different tissue characteristics, and together they allow radiologists to identify or exclude a wide range of pathological conditions. On a normal scan, each sequence produces predictable signal patterns that experienced readers recognize instantly.
For MRI technologists preparing for the ARRT registry examination, mastering the appearance of normal brain anatomy across multiple pulse sequences is a non-negotiable competency. The exam tests knowledge of normal anatomy extensively, and questions about what constitutes a normal versus abnormal finding appear consistently across test administrations. Knowing your baseline is the foundation upon which pathology recognition is built — you cannot identify what is wrong if you do not know precisely what is right.
The brain is divided into several major compartments that must each be systematically assessed. The supratentorial compartment houses the cerebral hemispheres, basal ganglia, thalami, and the lateral and third ventricles. The infratentorial compartment, or posterior fossa, contains the cerebellum, pons, medulla, and fourth ventricle. A complete MRI brain report addresses both compartments along with the extra-axial spaces, skull base, orbits (if included), and paranasal sinuses visible on the field of view.
Patients often feel anxious while waiting for MRI brain results, particularly when the scan was ordered to evaluate headaches, dizziness, memory changes, or neurological symptoms. When the radiologist reports a normal MRI brain, it means that no acute intracranial abnormality — such as hemorrhage, infarction, mass, or significant white matter disease — has been identified. This finding, while relieving, does not exclude every possible neurological condition, as some disorders (certain epilepsies, migraines, early neurodegenerative changes) may not produce visible MRI abnormalities.
From a clinical education standpoint, learning to read a brain MRI systematically is far more effective than trying to pattern-match individual findings. Radiologists and technologists alike are trained to follow a structured review approach: start with the sequences, assess brain parenchyma by region, evaluate the ventricular system, inspect the extra-axial spaces, examine vascular structures, and review the skull and scalp. This methodical approach prevents errors of omission and builds the systematic thinking that serves professionals throughout their careers. Resources like normal mri brain guides complement your understanding of adjacent spinal neuroimaging that pairs naturally with intracranial studies.
This comprehensive guide walks through every major element of a normal brain MRI, from sequence-by-sequence signal characteristics to age-related changes that are expected rather than pathological. Whether you are a patient trying to understand your radiology report, a student preparing for boards, or a technologist brushing up on fundamentals, this resource delivers the detailed, clinically accurate information you need.
Normal Brain MRI by the Numbers
Normal Brain MRI Anatomy by Region
On a normal brain MRI, the cortex appears as a thin gray ribbon outlining the gyri. Gray matter is isointense to slightly hypointense on T1 relative to white matter, while white matter appears brighter on T1 due to its higher myelin and lipid content.
The caudate nucleus, putamen, globus pallidus, and thalami form the deep gray matter structures. On T2-weighted images, the globus pallidus normally appears slightly hypointense due to iron deposition, which is an expected finding in adults over 25 years of age.
The four ventricles — two lateral, one third, one fourth — contain cerebrospinal fluid (CSF). On a normal brain MRI, CSF appears uniformly dark on T1, bright on T2, and suppressed (dark) on FLAIR. Symmetric ventricle size appropriate for age is a key normal finding.
The cerebellum shows normal foliar architecture with intact gray-white differentiation. The brainstem — midbrain, pons, and medulla — appears homogeneous without focal signal abnormality. The fourth ventricle sits midline and symmetrically positioned without displacement.
Normal sulci and cisterns contain CSF and should be symmetric. The meninges are not normally visible on standard sequences without contrast. After gadolinium, very thin, uniform dural enhancement can be a normal variant, but leptomeningeal enhancement is always abnormal.
Understanding MRI sequences and their corresponding normal signal patterns is the cornerstone of brain MRI interpretation. The four sequences used in virtually every standard brain MRI protocol — T1-weighted imaging, T2-weighted imaging, FLAIR (Fluid-Attenuated Inversion Recovery), and Diffusion-Weighted Imaging (DWI) — each exploit different tissue properties to generate contrast. On T1-weighted images, structures with short T1 relaxation times appear bright (hyperintense), while those with long T1 times appear dark. Fat, subacute blood products, and proteinaceous fluid are characteristically bright on T1, which is why these sequences are excellent for detecting subacute hemorrhage and assessing anatomy.
T2-weighted imaging reverses much of this contrast: fluid appears bright on T2 because water has a long T2 relaxation time. In a normal brain, the ventricles and subarachnoid spaces filled with CSF are uniformly bright on T2. Gray matter is slightly brighter than white matter on T2 because of its higher water content. Pathological processes that increase tissue water content — edema, inflammation, demyelination, early infarction — appear as T2 hyperintensities, making this sequence the most sensitive for detecting abnormality. A normal T2 brain scan shows no unexpected regions of abnormal signal within the parenchyma.
FLAIR is a T2-based sequence with an inversion pulse that nulls the signal from free water (CSF), causing it to appear dark. This suppression of CSF signal makes FLAIR extraordinarily sensitive for detecting periventricular and cortical lesions that might otherwise be obscured by adjacent bright CSF on standard T2 images.
On a normal brain FLAIR, the ventricles and cisterns are dark, while the cortex and white matter show expected low-to-intermediate signal. Occasional punctate or linear white matter foci on FLAIR in adults over 50 may represent normal small vessel ischemic changes, but their absence is the baseline expectation in younger patients.
Diffusion-weighted imaging (DWI) and its paired sequence, the apparent diffusion coefficient (ADC) map, are primarily used to detect acute ischemic stroke, in which the rapid movement of water from the extracellular to intracellular compartment restricts diffusion. On a normal DWI sequence, the brain parenchyma shows no areas of restricted diffusion. The ADC map should mirror the DWI — areas that are bright on DWI with corresponding low signal on ADC confirm true restricted diffusion, which is pathological. Areas that are bright on DWI but also bright on ADC represent T2 shine-through, a normal variant finding that does not indicate pathology.
Gadolinium-based contrast agents are not part of every brain MRI protocol, but when administered, they highlight disruptions in the blood-brain barrier (BBB). A normal post-contrast brain MRI shows enhancement of the choroid plexus, pituitary gland, dural venous sinuses, and nasal mucosa — these structures normally lack a BBB or have fenestrated endothelium. Brain parenchyma itself should not enhance in a normal study. Enhancement within the parenchyma signals BBB breakdown due to neoplasia, infection, active demyelination, or subacute infarction, all of which are abnormal findings requiring further workup.
Susceptibility-Weighted Imaging (SWI) is increasingly included in brain MRI protocols, particularly at 3 Tesla field strengths. SWI is exquisitely sensitive to substances that distort the local magnetic field — primarily blood products, calcium, and iron. On a normal brain SWI, the cortical and medullary veins appear as thin dark structures (hypointense) following an expected anatomical distribution.
Small foci of hypointensity in the basal ganglia represent normal iron deposition. The absence of unexpected low-signal foci scattered throughout the brain parenchyma is a key normal finding on SWI, as such foci would suggest microhemorrhages (microbleeds) seen in cerebral small vessel disease or amyloid angiopathy.
MRI spectroscopy (MRS), arterial spin labeling (ASL), and functional MRI (fMRI) are advanced techniques used in specific clinical contexts but are not part of the routine brain protocol. When MRS is performed, a normal spectrum shows characteristic peaks for N-acetylaspartate (NAA), choline, creatine, and sometimes lactate and lipids. A normal NAA peak, representing neuronal integrity, should be the tallest peak in healthy brain tissue. Elevation of choline relative to NAA, or the presence of a lactate peak, are abnormal spectroscopic findings associated with tumor and ischemia respectively.
MRI Practice Test Questions
Prepare for the MRI - Magnetic Resonance Imaging exam with our free practice test modules. Each quiz covers key topics to help you pass on your first try.
MRI Knowledge
MRI Exam Questions covering Knowledge. Master MRI Test concepts for certification prep.
MRI Physics
Free MRI Practice Test featuring Physics. Improve your MRI Exam score with mock test prep.
MRI Anatomy and Pathology
MRI Test Prep for MRI Anatomy and Pathology. Practice MRI Quiz questions and boost your score.
MRI Anatomy and Positioning
MRI Questions and Answers on MRI Anatomy and Positioning. Free MRI practice for exam readiness.
MRI Contrast Agents
Free MRI Quiz on MRI Contrast Agents. MRI Exam prep questions with detailed explanations.
MRI Patient Care and Positioning
MRI Practice Questions for MRI Patient Care and Positioning. Build confidence for your MRI certification exam.
T1, T2, and FLAIR: What Normal Brain MRI Looks Like
On T1-weighted images, normal brain anatomy is displayed with excellent gray-white matter differentiation. White matter appears hyperintense (bright) relative to gray matter because of its high myelin and lipid content, which shortens T1 relaxation time. The cortex forms a thin, intermediate-signal ribbon around the gyri. CSF in the ventricles and sulci appears uniformly dark (hypointense), providing a natural contrast boundary. The corpus callosum appears as a continuous bright white structure connecting the hemispheres, with well-defined genu, body, and splenium segments.
The deep gray matter structures — caudate, putamen, thalamus — appear isointense to cortical gray matter on T1. The posterior limb of the internal capsule is distinctly bright on T1 in newborns and infants due to early myelination, but in adults it blends with surrounding myelinated white matter. Fat-containing structures such as the marrow of the calvarium appear bright on T1. The pituitary gland normally shows a bright spot in its posterior lobe on T1, representing neurosecretory granules, and this finding is expected in normal adults.

Brain MRI vs. CT: Advantages and Limitations for Normal Brain Evaluation
- +Superior soft tissue contrast reveals subtle gray-white matter differentiation not visible on CT
- +No ionizing radiation, making it safe for repeated imaging and pediatric patients
- +Multiplanar capability allows axial, coronal, and sagittal views without repositioning
- +Sensitive to early ischemic change on DWI long before CT shows abnormality
- +FLAIR detects periventricular and cortical lesions obscured by CSF on other modalities
- +Excellent for posterior fossa imaging without bone artifact that limits CT in that region
- −Longer acquisition time (30–60 min) increases motion artifact risk compared to CT (seconds)
- −Contraindicated for patients with certain metallic implants, pacemakers, or cochlear implants
- −Claustrophobia and patient anxiety can limit image quality or require sedation
- −Less sensitive than CT for acute subarachnoid hemorrhage within the first 24 hours
- −Higher cost and less widely available than CT, particularly in emergency settings
- −Calcium and acute bone abnormalities are less well-visualized on MRI than CT
Reading a Normal Brain MRI: Systematic Review Checklist
- ✓Confirm correct patient, date, field strength, and sequences before reviewing images
- ✓Assess overall brain size and morphology relative to the patient's stated age
- ✓Evaluate gray-white matter differentiation on T1 throughout both hemispheres
- ✓Inspect all white matter for T2 or FLAIR hyperintensities, noting size and distribution
- ✓Review the ventricular system for appropriate size, symmetry, and CSF signal uniformity
- ✓Examine the corpus callosum in its entirety — genu, body, and splenium — on sagittal T1
- ✓Assess the posterior fossa including cerebellum, brainstem, and fourth ventricle position
- ✓Confirm presence of normal flow voids in the major intracranial arteries and dural sinuses
- ✓Inspect the DWI sequence for any areas of restricted diffusion with ADC confirmation
- ✓Review extra-axial spaces for symmetric sulci and absence of collections or enhancement
A Normal MRI Does Not Rule Out All Neurological Conditions
While a normal brain MRI is highly reassuring, certain neurological conditions — including idiopathic epilepsy, migraine without aura, early Parkinson's disease, and functional neurological disorder — may produce no detectable MRI abnormalities. Clinical correlation remains essential, and a normal scan should be interpreted in context with the patient's full symptom picture and examination findings.
Distinguishing normal age-related brain changes from true pathological findings is one of the most clinically important skills in brain MRI interpretation. The brain undergoes predictable changes throughout the lifespan that must be recognized as expected rather than alarming. In neonates, the brain is predominantly unmyelinated, causing most white matter to appear dark on T1 and bright on T2 — essentially the opposite of adult signal patterns.
Myelination progresses in a predictable sequence from dorsal to ventral, caudal to cranial, and central to peripheral, completing by approximately age 2 years. Pediatric brain MRI interpretation therefore requires comparing findings to published myelination milestones.
In young and middle-aged adults, the white matter should appear homogeneous and clean on all sequences. The ventricles are relatively small, the sulci are narrow, and the brain parenchyma fills the calvarium with only minimal extra-axial CSF spaces. As adults enter their 40s and 50s, the first age-related changes begin to appear. Mild widening of the sulci and slight increase in ventricular size reflect the earliest stages of age-related volume loss. These findings are considered normal when mild and symmetric, and should prompt no clinical alarm in the absence of cognitive symptoms.
White matter signal changes on FLAIR deserve special attention in older adults because they are among the most common MRI findings in the population over age 60. Small scattered punctate white matter hyperintensities (WMH) distributed in the periventricular and subcortical regions are classified using standardized grading systems such as the Fazekas scale. Fazekas 0 (no WMH) and Fazekas 1 (punctate foci) are generally considered within the spectrum of normal aging. Fazekas 2 (beginning confluence) and Fazekas 3 (large confluent areas) represent increasing degrees of small vessel ischemic disease and are associated with vascular risk factors and cognitive decline.
Iron deposition in the deep gray matter structures is another expected age-related finding that accumulates progressively throughout adulthood. The globus pallidus, substantia nigra, red nucleus, and dentate nucleus all accumulate iron as part of normal physiology, appearing hypointense on T2 and GRE/SWI sequences. This normal iron deposition should not be confused with pathological hypointensity from microhemorrhages, which tend to cluster in different distributions and are associated with hypertension or cerebral amyloid angiopathy.
Enlarged perivascular spaces (EPVS), also called Virchow-Robin spaces, are CSF-filled spaces surrounding perforating arteries as they enter the brain parenchyma. On MRI, they appear as small, linear or oval structures following CSF signal on all sequences — dark on T1, bright on T2, and dark on FLAIR. Their FLAIR suppression is the key feature distinguishing them from white matter lesions, which remain bright on FLAIR. Mild EPVS in the basal ganglia and white matter are a normal finding in adults of all ages; prominent EPVS in the elderly may reflect small vessel disease but are generally not individually pathological.
The choroid plexus, located within the lateral, third, and fourth ventricles, produces CSF and normally appears as lobulated soft tissue with avid enhancement after gadolinium. Choroid plexus calcifications are extremely common in adults and appear as hypointense foci on MRI (better seen on CT). These calcifications are benign and should be distinguished from the rare choroid plexus papilloma or carcinoma, which presents as an enhancing mass causing hydrocephalus.
Arachnoid cysts are another common incidental finding — extra-axial collections that follow CSF signal on all sequences, including FLAIR suppression, and do not enhance. They are developmental variants found in 1–2% of the population and require no intervention when asymptomatic.
Pineal cysts represent another frequent incidental brain MRI finding, occurring in up to 4% of adult scans. A normal pineal cyst is small (under 10–15mm), has thin smooth walls, and follows CSF signal characteristics. Larger cysts or those with thick walls, internal septations, or solid nodular components warrant additional evaluation. Similarly, small pituitary cysts and Rathke's cleft cysts are incidental findings that are benign when they lack mass effect on the optic chiasm or other pituitary structures. Recognizing these common normal variants prevents unnecessary patient anxiety and additional costly workup.

Not every brain MRI requires gadolinium contrast. Routine brain MRI for headache evaluation, first seizure, or screening purposes is typically performed without contrast. Contrast is added when evaluating for tumor, infection, active demyelination, vasculitis, or leptomeningeal disease. Always verify your facility's protocol and whether the ordering physician has specified with or without contrast before beginning the scan.
For MRI technologists preparing for the ARRT registry examination, a thorough knowledge of normal brain MRI is tested both directly and indirectly across multiple content domains. The registry examination includes questions on normal anatomy identification, pulse sequence selection and their effects on tissue contrast, artifact recognition, patient safety, and protocol optimization. Questions about the brain represent a significant portion of the anatomy and pathology content domain, making brain MRI one of the highest-yield areas for exam preparation. Students who invest time mastering normal brain anatomy across all standard sequences consistently outperform those who focus exclusively on pathological conditions.
The ARRT MRI examination tests anatomical knowledge at the level of named structures, tracts, and landmarks. For the brain, candidates are expected to identify major sulci and gyri (central sulcus, lateral sulcus, calcarine fissure), deep structures (caudate, putamen, globus pallidus, internal capsule divisions, thalamus, hippocampus, amygdala), brainstem subdivisions (midbrain, pons, medulla with their associated cranial nerve nuclei), cerebellar anatomy (vermis, hemispheres, flocculonodular lobe, dentate nuclei), and the cranial nerve exit zones. Being able to locate these structures on MRI images in axial, coronal, and sagittal planes is a core competency.
Pulse sequence physics questions on the registry examination frequently use brain MRI examples to test understanding of TR, TE, TI (inversion time), flip angle, and their effects on tissue contrast. Understanding why CSF appears dark on T1, bright on T2, and suppressed on FLAIR — and being able to explain the physical basis for each — demonstrates the integrated knowledge that the examination rewards. Similarly, understanding why certain sequences are selected for specific clinical questions (DWI for acute stroke, FLAIR for MS plaques, GRE or SWI for hemorrhage detection) shows the clinical reasoning skills that distinguish competent technologists.
Artifacts are another critical brain MRI topic. Motion artifact is the most common source of image degradation in brain MRI and appears as ghosting or blurring in the phase-encoding direction. Susceptibility artifact from dental hardware, surgical clips, or hemorrhage causes focal signal dropout and distortion, particularly on gradient echo and EPI-based sequences like DWI.
Chemical shift artifact creates bright and dark bands at fat-water interfaces, visible at the skull base and orbits. Gibbs ringing (truncation artifact) produces parallel lines near sharp tissue interfaces and is commonly seen at the brain-CSF boundary. Recognizing artifacts prevents misidentification as pathology and is tested directly on the ARRT exam.
MRI safety knowledge directly intersects with brain MRI in several important ways. The presence of cerebral aneurysm clips, cochlear implants, deep brain stimulators, and certain vascular access devices may be absolute or relative contraindications to brain MRI. Technologists must be proficient in screening patients for these implants before positioning them near the magnet. The force and torque exerted by a strong magnetic field on ferromagnetic implants can cause catastrophic injury, particularly for intracranial devices adjacent to sensitive neural structures. Always verify implant safety using current manufacturer MRI compatibility documentation and resources such as MRIsafety.com.
Study strategies for normal brain MRI on the registry exam should include systematic image review sessions using practice images, flashcard systems for signal intensities across sequences, and timed practice questions that mirror the exam format. Many candidates find it helpful to draw brain anatomy diagrams from memory and then verify accuracy against atlas images.
Understanding the embryological basis for brain development also helps with questions about developmental anomalies that must be distinguished from acquired pathology on normal versus abnormal scans. Consistent, spaced repetition of anatomy facts over weeks rather than cramming in the final days produces the most durable retention of complex neuroanatomical information.
Connecting theoretical knowledge to the practical scanning environment is equally important for registry readiness. Technologists who understand why each sequence is prescribed — not just how to prescribe it — can troubleshoot protocol deviations, adapt when patients cannot cooperate fully, and recognize when image quality is insufficient for diagnostic interpretation.
This clinical judgment, built on a foundation of normal brain MRI knowledge, is precisely what the registry examination assesses and what distinguishes highly competent MRI technologists in practice. Resources like our normal mri brain related guides extend this foundational knowledge into adjacent imaging areas that frequently appear on the same examination day.
Practical preparation for reading normal brain MRI scans requires more than textbook study — it demands regular exposure to actual imaging cases across a range of patient ages, field strengths, and protocol variations. One of the most effective strategies is systematic case review using publicly available teaching files, radiology education platforms, and institutional case libraries.
Setting a daily goal of reviewing a defined number of normal brain MRI scans before progressing to pathological cases builds the visual memory foundation that makes abnormalities immediately recognizable by contrast. Experienced radiologists describe the process of reading a normal scan not as an absence of findings, but as an active confirmation that every structure looks exactly as expected.
Field strength awareness is practically important when interpreting or producing brain MRI images. At 1.5 Tesla, images have lower intrinsic SNR (signal-to-noise ratio), which translates to lower spatial resolution or longer scan times to achieve comparable image quality. At 3 Tesla, the doubled SNR can be invested in higher spatial resolution, thinner slices, or shorter scan times, all of which benefit brain imaging.
However, 3T also amplifies susceptibility effects, chemical shift artifact, and SAR (specific absorption rate) deposition. Understanding these tradeoffs helps technologists optimize protocols and explain image characteristics to referring physicians who may question why a scan obtained at one field strength looks different from one at another.
Patient positioning and head coil selection significantly influence normal brain MRI image quality. Standard brain MRI uses a dedicated head coil (typically 8-channel or higher) with the patient supine, head centered in the coil, and the Frankfurt plane (a line from the ear canal to the lower orbital rim) perpendicular to the patient table.
Proper head positioning ensures that axial slices are acquired parallel to the anterior-posterior commissure line, which is the standard anatomical reference plane for brain MRI. Deviation from this plane changes the apparent anatomy of structures like the hippocampus, temporal lobes, and brainstem, potentially creating pseudo-abnormalities or obscuring real findings.
Slice thickness selection is a practical decision with real consequences for normal brain MRI interpretation. Routine brain MRI typically uses 4–5mm axial slices with a 1mm interslice gap for conventional sequences, but high-resolution volumetric acquisitions (such as 3D MPRAGE for T1 or 3D FLAIR) obtain 1mm isotropic voxels that can be reformatted in any plane.
Thicker slices reduce spatial resolution and increase partial volume averaging, which can obscure small cortical lesions, tiny cavernous malformations, or thin subdural collections. When imaging is performed to evaluate a specific small structure — the pituitary gland, internal auditory canals, or hippocampi for seizure workup — dedicated thin-slice sequences are added to the standard protocol.
Contrast timing and dose are important technical considerations when gadolinium is administered for brain MRI. The standard dose of gadolinium-based contrast agent (GBCA) is 0.1 mmol/kg body weight for conventional brain MRI. Higher doses (0.2–0.3 mmol/kg) are sometimes used for specific indications such as detection of small brain metastases or leptomeningeal disease.
Post-contrast T1 images should be obtained within a specific time window after injection — typically 5–10 minutes — to optimize enhancement of lesions while minimizing the risk of missing early or transient enhancement. Delayed images at 10–20 minutes after injection can increase sensitivity for certain pathologies, including infectious meningitis and small metastases.
Reporting a normal brain MRI follows a standardized structure that ensures all relevant areas are addressed. A typical radiology report for a normal brain MRI includes the clinical indication, technique (sequences performed, field strength, use of contrast), findings (systematically organized by brain region), and impression (concise summary statement). The impression for a truly normal study often reads: 'No acute intracranial abnormality identified. Normal MRI of the brain without/with contrast.' This statement carries significant diagnostic weight, confirming to the clinician that the differential diagnosis should be redirected away from structural pathology toward functional, metabolic, or systemic etiologies.
For patients receiving a normal brain MRI report, understanding what this finding means — and what it does not exclude — is an important component of the clinical consultation. A normal MRI rules out structural causes of symptoms detectable at the field strength and with the protocol used, but it cannot exclude every possible neurological condition.
Functional MRI symptoms, psychogenic disorders, certain metabolic encephalopathies, and very early degenerative diseases may produce no MRI-visible abnormality. Patients should be encouraged to discuss the interpretation of their results with their ordering physician, who can place the imaging findings in the full context of their clinical presentation, laboratory results, and neurological examination.
MRI Questions and Answers

MRI of Cervical Spine: Complete Guide to Imaging, Anatomy, Pathology, and Patient Preparation

Knee MRI Images: A Complete Guide to Reading, Understanding, and Interpreting Knee Scans
Ace Your Exam with MRI Practice Test 2026 Prep

MRI Tech School 2026 — Programs, Requirements, and What to Expect
MRI Procedure: What to Expect Before, During and After Your Scan
About the Author

Medical Laboratory Scientist & Clinical Certification Expert
Johns Hopkins UniversityDr. Sandra Kim holds a PhD in Clinical Laboratory Science from Johns Hopkins University and is certified as a Medical Technologist (MT) and Medical Laboratory Scientist (MLS) through ASCP. With 16 years of clinical laboratory experience spanning hematology, microbiology, and molecular diagnostics, she prepares candidates for ASCP board exams, MLT, MLS, and specialist certification tests.
Join the Discussion
Connect with other students preparing for this exam. Share tips, ask questions, and get advice from people who have been there.
View discussion (6 replies)