Does Your Whole Body Go In for a Brain MRI? What to Expect Before, During, and After Your Scan
🗨️ Does your whole body go in for a brain MRI? Learn exactly what happens, how far you slide in, and how to prepare for your scan.

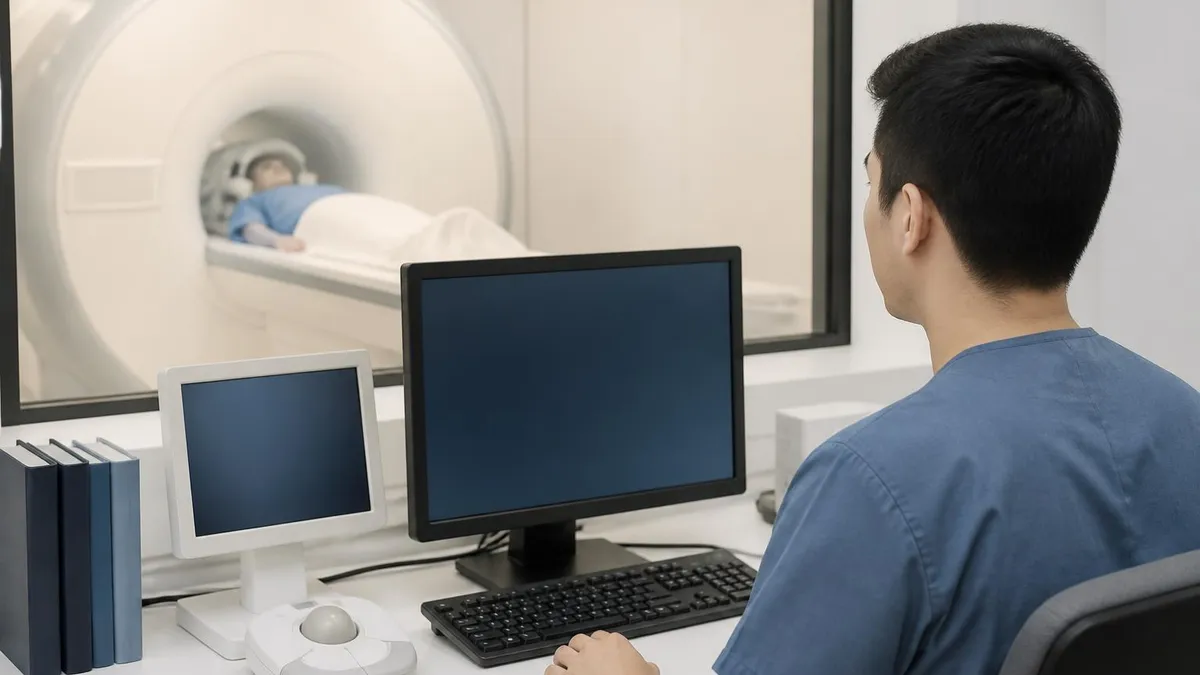
If you've been scheduled for a brain MRI, you've probably wondered: does your whole body go in for a brain MRI? The short answer is yes — in most standard closed-bore scanners, your entire body slides into the tube, even though only your head and brain are being imaged. This happens because the machine needs your head centered precisely inside the magnetic coil, and the table must slide far enough inward to position your skull within the strongest part of the magnetic field.
Understanding exactly what to expect during a brain mri procedure can dramatically reduce the anxiety many patients feel before their appointment. Claustrophobia is one of the most common concerns radiologists and MRI technologists hear, and knowing the mechanics of the machine helps patients prepare mentally. You'll enter the scanner feet-first, and depending on your height, your feet and lower legs may actually remain outside the bore of the magnet entirely.
A brain MRI uses powerful magnetic fields — typically 1.5 Tesla or 3 Tesla — and radio waves to produce detailed images of brain tissue, blood vessels, and cerebrospinal fluid. The scan can detect tumors, strokes, aneurysms, multiple sclerosis lesions, and dozens of other neurological conditions with extraordinary clarity. No radiation is involved, which is one reason doctors prefer MRI over CT scanning for repeated imaging of the brain.
Before the scan begins, you'll be asked to remove all metal objects from your body and answer a safety screening questionnaire. Metal implants, pacemakers, cochlear implants, and certain surgical clips can be dangerous near the MRI magnet, so full disclosure is essential. The technologist will ask about prior surgeries, implants, tattoos with metallic ink, and any history of working with metal. This screening is non-negotiable and exists entirely for your protection.
The duration of a brain MRI typically ranges from 30 to 60 minutes, though some specialized protocols — such as functional MRI (fMRI) or spectroscopy — can extend the session to 90 minutes or more. During that time, you'll need to remain as still as possible. Even small head movements can blur the images enough to require the sequence to be repeated, prolonging your time in the scanner. Earplugs or headphones are provided because the machine produces loud banging and clicking sounds throughout the scan.
Some brain MRIs require contrast enhancement using a gadolinium-based agent injected through an IV line. Gadolinium lights up areas of abnormal blood-brain barrier breakdown, making tumors, active inflammation, and certain vascular abnormalities far more visible. Your ordering physician will specify whether contrast is needed based on your clinical situation. If contrast is ordered, a nurse or technologist will place an IV catheter in your arm before you enter the scanner room.
After the scan, most patients resume normal activities immediately — there's no recovery period, no lingering sedation (unless you requested anti-anxiety medication), and no radiation exposure to worry about. A radiologist will analyze the images and send a report to your doctor, typically within 24 to 72 hours. Understanding the full arc of the experience — from arrival to results — helps patients approach the appointment with confidence rather than dread.
Brain MRI by the Numbers

How the MRI Machine Positions Your Body During a Brain Scan
Arrival and Check-In
Positioning on the Table
Sliding Into the Bore
Imaging Sequences Begin
Contrast Injection (If Ordered)
Table Withdrawal and Completion
Preparing for a brain MRI correctly makes a meaningful difference in both image quality and your personal comfort during the scan. The most important preparation step is understanding which personal items and implants are incompatible with the MRI environment. The magnetic field in an MRI scanner is always on — it never turns off — so even walking into the room with a ferromagnetic object can be dangerous. Jewelry, belt buckles, underwire bras, hairpins, and hearing aids must all be removed before you approach the scanner.
Dietary restrictions for a brain MRI are minimal compared to other procedures. In most cases, you can eat and drink normally before the scan unless your facility asks you to fast if sedation is planned. If your physician has ordered gadolinium contrast and you have a history of kidney disease, you may need recent lab work showing your kidney function before the injection is approved. Gadolinium is cleared by the kidneys, and patients with severe renal impairment face a small risk of a rare condition called nephrogenic systemic fibrosis.
Clothing choices matter more than most patients realize. Avoid wearing clothes with metal snaps, zippers, or underwire support. Many facilities will ask you to change into a hospital gown regardless, but wearing loose, metal-free clothing like athletic wear can sometimes allow you to remain dressed during the scan, which many patients find more comfortable. Leave watches, earrings, and piercings at home rather than trying to remove them on-site.
If you take regular medications, continue them as normal unless your physician instructs otherwise. Anti-anxiety medications such as lorazepam or diazepam are sometimes prescribed for patients with moderate claustrophobia, but you must arrange a driver since you cannot legally drive after taking a benzodiazepine. Inform the MRI facility at scheduling that you anticipate needing medication — they can coordinate with your ordering physician and ensure the prescription is in place before your appointment day.
Patients with tattoos should inform the technologist before the scan. A small number of older tattoo inks contain metallic particles that can cause localized warmth or tingling during the scan. Modern tattoo inks are generally safe, but it's worth disclosing so the team can monitor your comfort. Similarly, patients with permanent cosmetic makeup — such as tattooed eyeliner — should mention this during screening.
Pediatric patients and adults with cognitive impairments may require general anesthesia rather than conscious sedation to keep the head perfectly still during the scan. Motion artifact in pediatric brain MRI is a significant quality issue, and anesthesia allows the team to acquire clean images in a single session rather than repeating sequences multiple times. When anesthesia is involved, fasting requirements (nothing by mouth for six to eight hours) apply strictly.
Finally, plan your arrival time with a buffer. MRI schedules frequently run 15 to 30 minutes late due to prior patients with complex anatomy or scan extensions. Arriving stressed and rushing to complete paperwork adds unnecessary anxiety. Give yourself at least 20 extra minutes beyond your scheduled appointment time, and bring something to read or listen to while you wait in the pre-scan area.
MRI Practice Test Questions
Prepare for the MRI - Magnetic Resonance Imaging exam with our free practice test modules. Each quiz covers key topics to help you pass on your first try.
MRI Knowledge
MRI Exam Questions covering Knowledge. Master MRI Test concepts for certification prep.
MRI Physics
Free MRI Practice Test featuring Physics. Improve your MRI Exam score with mock test prep.
MRI Anatomy and Pathology
MRI Test Prep for MRI Anatomy and Pathology. Practice MRI Quiz questions and boost your score.
MRI Anatomy and Positioning
MRI Questions and Answers on MRI Anatomy and Positioning. Free MRI practice for exam readiness.
MRI Contrast Agents
Free MRI Quiz on MRI Contrast Agents. MRI Exam prep questions with detailed explanations.
MRI Patient Care and Positioning
MRI Practice Questions for MRI Patient Care and Positioning. Build confidence for your MRI certification exam.
What Happens Inside the MRI Scanner: Sequences, Sounds, and Sensations
A brain MRI is not a single image — it's a series of pulse sequences, each designed to highlight different tissue characteristics. T1-weighted images show anatomy clearly and are best for identifying structural abnormalities. T2-weighted images make fluid bright, which is ideal for detecting edema, demyelination, and most lesions. FLAIR (Fluid-Attenuated Inversion Recovery) suppresses cerebrospinal fluid signal to make periventricular lesions far more conspicuous than on standard T2 images.
Diffusion-weighted imaging (DWI) detects the random Brownian motion of water molecules and is the sequence of choice for diagnosing acute ischemic stroke, sometimes identifying infarction within minutes of symptom onset. Susceptibility-weighted imaging (SWI) is exquisitely sensitive to blood products, calcium, and iron, making it valuable for detecting microbleeds, cavernous malformations, and hemorrhagic transformation. Your radiologist selects sequences based on your clinical indication — a stroke workup looks very different from a seizure protocol.

Brain MRI vs. CT Scan: Which Is Better for Brain Imaging?
- +Superior soft tissue contrast for detecting small lesions, white matter changes, and cortical pathology
- +No ionizing radiation, making it safe for repeated imaging and in pediatric patients
- +Multiplanar capability — images acquired directly in axial, coronal, and sagittal planes without repositioning
- +Functional sequences (fMRI, DWI, MRS) provide physiologic information beyond pure anatomy
- +Excellent for posterior fossa and brainstem imaging without the beam-hardening artifact that degrades CT in this region
- +Gadolinium contrast has a superior safety profile compared to iodinated CT contrast in patients with mild-to-moderate kidney disease
- −Significantly longer scan time (30–60 min) versus CT (5–10 min), problematic for unstable or uncooperative patients
- −Higher cost — brain MRI typically runs $1,000–$3,000 versus $300–$700 for a head CT without insurance
- −Contraindicated in patients with many implanted devices including older pacemakers, cochlear implants, and ferromagnetic aneurysm clips
- −Claustrophobia affects 5–10% of patients and may require sedation or open-MRI alternatives
- −Poorer sensitivity for acute subarachnoid hemorrhage compared to non-contrast head CT in the first 24 hours
- −Motion artifact degrades image quality significantly more than in CT, often requiring repeat sequences
Brain MRI Preparation Checklist: 10 Steps Before Your Appointment
- ✓Disclose all metal implants, surgical hardware, and pacemakers to your ordering physician and the MRI facility at the time of scheduling.
- ✓Confirm whether contrast (gadolinium) is ordered and ask your doctor if recent kidney function labs are required.
- ✓Arrange a designated driver if you plan to take anti-anxiety medication before the scan.
- ✓Wear loose, metal-free clothing such as athletic pants and a cotton shirt with no underwire or metal fasteners.
- ✓Remove all jewelry, piercings, and hair accessories the morning of your appointment — leave them at home.
- ✓Eat and drink normally unless your facility specifically instructs you to fast for sedation.
- ✓Arrive at least 20 minutes early to complete safety screening paperwork without feeling rushed.
- ✓Inform the technologist of any tattoos, permanent cosmetic makeup, or history of working with metal shavings.
- ✓Practice slow, diaphragmatic breathing before the scan to activate the parasympathetic nervous system and reduce claustrophobic anxiety.
- ✓Ask the technologist for a verbal countdown before each sequence begins so you know exactly how long you need to stay still.
Claustrophobic? An Open or Wide-Bore MRI May Be Available
Wide-bore MRI scanners (70 cm diameter vs. the standard 60 cm) and open MRI units reduce claustrophobia significantly. Wide-bore 3T systems now match closed-bore image quality while giving patients noticeably more breathing room. Ask your radiology facility which scanner configurations are available before your appointment — most facilities can accommodate claustrophobic patients with the right equipment or sedation protocol.
One of the most compelling reasons physicians order brain MRI over other imaging modalities is its extraordinary range of detectable pathologies. The brain is among the most diagnostically complex organs in the body, and MRI's combination of tissue contrast, multiplanar imaging, and functional sequences makes it uniquely suited to evaluating nearly every category of neurological disease. Understanding what conditions can and cannot be detected on brain MRI helps patients contextualize their results when the radiologist's report arrives.
Ischemic stroke is one of the most time-sensitive diagnoses in all of medicine, and diffusion-weighted MRI can detect acute infarction within minutes to hours of symptom onset — far earlier than CT, which typically shows no abnormality in the first 24 hours. DWI detects the restriction of water diffusion in cells that have suffered acute ischemic injury, producing a bright signal in the affected territory. This early detection capability is why stroke centers now run MRI protocols concurrently with CT angiography for the most comprehensive acute stroke workup.
Primary brain tumors — including glioblastoma multiforme, oligodendroglioma, meningioma, and ependymoma — each display characteristic signal patterns on standard brain MRI sequences. Gadolinium enhancement patterns, mass effect, surrounding edema, and the T1/T2 signal profile all contribute to narrowing the differential diagnosis before tissue biopsy. MRI also guides stereotactic biopsy planning by defining the tumor's relationship to eloquent cortex and white matter tracts that control movement and language.
Multiple sclerosis (MS) is perhaps the neurological condition most closely associated with brain MRI in the public consciousness. MS demyelinating plaques appear as ovoid white matter lesions on T2 and FLAIR sequences, classically perpendicular to the corpus callosum — the so-called Dawson's fingers pattern. Gadolinium-enhancing lesions indicate active inflammation through a disrupted blood-brain barrier and are critical for determining disease activity status, distinguishing new from old lesions, and monitoring treatment response in patients on disease-modifying therapies.
Infectious and inflammatory conditions of the brain are also well-characterized on MRI. Bacterial meningitis produces pachymeningeal or leptomeningeal enhancement on post-contrast sequences. Herpes simplex encephalitis shows characteristic signal abnormality in the temporal lobes before systemic symptoms fully manifest. Cerebral abscess displays ring enhancement with a restricted diffusion core — a pattern so specific it can be distinguished from cystic tumor on imaging alone in most cases, guiding antibiotic versus surgical management.
Vascular malformations including arteriovenous malformations (AVMs), cavernous malformations, and developmental venous anomalies all have distinctive MRI signatures. Susceptibility-weighted imaging is particularly sensitive for detecting small cavernous malformations and microbleeds that may be entirely invisible on CT. MR angiography (MRA) can visualize major intracranial vessels without contrast in many cases, providing a non-invasive alternative to conventional catheter angiography for initial vascular screening.
Neurodegenerative conditions such as Alzheimer's disease, frontotemporal dementia, and Parkinson's disease also produce characteristic structural changes detectable on brain MRI, including hippocampal atrophy, frontal lobe volume loss, and iron deposition in the basal ganglia. While MRI cannot definitively diagnose these conditions — that still requires clinical correlation and, increasingly, PET imaging with amyloid or tau tracers — it plays an essential role in ruling out structural causes of cognitive decline and quantifying disease progression over time.

Never assume an implant is MRI-safe without verification. Even devices marketed as 'MRI-compatible' may only be safe under specific field strength or time conditions. Bring implant cards, device manufacturer information, or surgical records to your appointment. The MRI technologist will verify compatibility using manufacturer databases before allowing you into the scanner room — this step cannot be skipped.
Managing claustrophobia and anxiety before and during a brain MRI is one of the most practical challenges both patients and MRI technologists face. Estimates suggest that between 5 and 10 percent of patients experience significant anxiety or claustrophobia during MRI scanning, and 1 to 2 percent are unable to complete the scan without pharmaceutical intervention. Understanding the full range of strategies available — from behavioral techniques to pharmacological support — means no patient should be forced to choose between their health and their comfort.
Cognitive preparation is the most underutilized anxiety management tool available to patients. The simple act of watching a video walkthrough of an MRI scan before your appointment — seeing the machine, hearing the sounds, observing what a real patient experiences — reduces anticipatory anxiety in controlled studies. Knowing that you have a call button in your hand, that the technologist can hear you at all times through a two-way intercom, and that you can request the scan be paused at any moment gives patients a genuine sense of agency over an experience that otherwise feels passive and confining.
Breathing techniques work in real time inside the scanner. Slow diaphragmatic breathing — inhaling for four counts, holding for two, exhaling for six — activates the parasympathetic nervous system and measurably reduces heart rate and cortisol levels within two to three minutes. Patients who practice this technique before the scan and use it actively during sequences report significantly lower distress than those who try to simply tolerate the experience without a strategy. Some facilities now provide guided audio breathing exercises through the in-bore headphones.
Prism glasses are a simple, low-tech solution that many MRI facilities offer on request. These angled lenses allow the patient to look through the bore of the magnet and see the room rather than staring at the ceiling inches above their face. For many mildly claustrophobic patients, the visual confirmation that they are not sealed inside a box — that there is open space visible beyond the tunnel — is sufficient to reduce anxiety to manageable levels without any medication whatsoever.
For patients with moderate to severe claustrophobia, oral benzodiazepines such as lorazepam (0.5–1 mg) or diazepam (5–10 mg) taken 30 to 60 minutes before the scan are highly effective. These medications produce sedation and anxiolysis without the risks of general anesthesia, and the vast majority of patients who use them complete their scans successfully. The critical planning requirement is arranging a driver, as you cannot operate a vehicle after taking a benzodiazepine. Discuss this option with your ordering physician at least 48 hours before your appointment so the prescription can be in place.
Wide-bore and open MRI alternatives should always be explored for patients with significant claustrophobia before concluding that sedation or anesthesia is necessary. Wide-bore 3 Tesla systems offer a 70 cm bore diameter versus the standard 60 cm, reducing the sense of confinement meaningfully while maintaining diagnostic image quality. Open MRI systems with a vertical or C-shaped magnet configuration eliminate the bore entirely but typically operate at lower field strengths (0.3–1.0 Tesla), which may limit the diagnostic value for certain brain protocols — your radiologist can advise on whether an open system is appropriate for your specific clinical question.
After the scan is complete, give yourself permission to decompress. Patients who experience even moderate anxiety during an MRI sometimes feel emotionally drained afterward, which is a completely normal physiological response to sustained stress. Schedule your appointment at a time when you can rest or take a quiet walk afterward rather than rushing immediately back to demanding obligations. Positive self-acknowledgment — recognizing that you successfully completed a medical procedure that felt challenging — reinforces your capacity to handle future imaging with increasing confidence.
For MRI technologists and radiology students, mastering the clinical nuances of brain MRI protocols is an essential step toward professional excellence and registry exam success. The brain MRI section of the ARRT MRI registry examination tests candidates on pulse sequence selection, artifact recognition, patient positioning, coil selection, contrast administration protocols, and safety screening procedures. Each of these domains maps directly to real clinical decisions made by technologists every day in the MRI suite.
Positioning accuracy is foundational. The head coil must be centered precisely within the bore so that the brain is located at the isocenter of the magnet — the point of maximum field homogeneity. Even a few centimeters of off-center positioning degrades image quality through B0 field inhomogeneity and gradient nonlinearity effects. The technologist uses anatomical landmarks — the nasion and external auditory meatus — to set the scan reference point before prescribing imaging planes on the localizer images.
Slice prescription for brain MRI follows standardized anatomical conventions. Axial slices are typically prescribed parallel to the anterior commissure-posterior commissure (AC-PC) line — a reference line visible on the sagittal localizer that standardizes slice position across patients and enables reproducible comparison on follow-up imaging. Coronal sequences are often prescribed perpendicular to the long axis of the hippocampus for optimal temporal lobe evaluation, particularly in epilepsy protocols. Sagittal sequences through the midline are essential for evaluating the corpus callosum, brainstem, and cerebellar vermis.
Artifact recognition is a critical competency that differentiates expert technologists from novices. Motion artifact — visible as ghosting or blurring in the phase-encode direction — is the most common image quality degrader in brain MRI and almost always reflects patient movement during the acquisition. Chemical shift artifact appears at fat-water interfaces and can obscure lesions adjacent to the scalp or orbit. Susceptibility artifact from metallic dental work, surgical clips, or blood products produces signal dropout and geometric distortion that can mimic or obscure pathology in adjacent brain tissue.
The ARRT MRI registry examination includes approximately 200 scored questions covering patient care, imaging procedures, and physical principles. Candidates have three hours to complete the exam and must achieve a minimum scaled score of 75 to pass. Historical first-time pass rates hover around 80 percent, but candidates who use structured practice testing — particularly question banks that mirror the registry's emphasis on clinical application rather than pure recall — consistently outperform those who rely on textbook reading alone.
Protocol optimization is an ongoing responsibility for MRI technologists working in busy brain imaging practices. As scanner hardware and software evolve, newer acquisition techniques such as simultaneous multislice imaging, compressed sensing, and deep learning image reconstruction are dramatically reducing scan times without compromising diagnostic quality. A brain MRI that took 45 minutes five years ago may now be completed in under 20 minutes on a modern platform — a change that improves patient throughput, reduces the likelihood of motion artifact from fatigue, and expands access for patients who struggle with extended scan durations.
Quality assurance responsibilities extend beyond individual patient scans. Technologists participate in phantom imaging programs that verify geometric accuracy, signal-to-noise ratios, and slice thickness consistency on a regular schedule. Accreditation by the American College of Radiology (ACR) requires documented QA protocols and periodic phantom scan review. Understanding these system-level responsibilities prepares registry candidates for questions about MRI quality management and regulatory compliance that appear on the examination.
Building a strong foundation in brain MRI fundamentals — from basic pulse sequence physics through clinical protocol design and patient care — is the bedrock of registry preparation. The most effective study approach combines structured review of physics principles, systematic anatomy study using real MRI images, and high-volume practice testing that simulates the cognitive demands of the actual examination. Technologists who engage actively with practice questions from day one of their preparation consistently develop stronger clinical reasoning than those who defer testing until the final weeks before their exam date.
MRI Questions and Answers

MRI of Cervical Spine: Complete Guide to Imaging, Anatomy, Pathology, and Patient Preparation

Knee MRI Images: A Complete Guide to Reading, Understanding, and Interpreting Knee Scans
Ace Your Exam with MRI Practice Test 2026 Prep

MRI Tech School 2026 — Programs, Requirements, and What to Expect
MRI Procedure: What to Expect Before, During and After Your Scan
About the Author

Medical Laboratory Scientist & Clinical Certification Expert
Johns Hopkins UniversityDr. Sandra Kim holds a PhD in Clinical Laboratory Science from Johns Hopkins University and is certified as a Medical Technologist (MT) and Medical Laboratory Scientist (MLS) through ASCP. With 16 years of clinical laboratory experience spanning hematology, microbiology, and molecular diagnostics, she prepares candidates for ASCP board exams, MLT, MLS, and specialist certification tests.
Join the Discussion
Connect with other students preparing for this exam. Share tips, ask questions, and get advice from people who have been there.
View discussion (6 replies)