24 Hour EEG: What to Expect, How It Works, Costs, and Results Explained
24 hour EEG test guide: what is an EEG test, how it works, cost, side effects, results, and tips to prepare for ambulatory monitoring at home. ⏳

A 24 hour EEG is an extended version of the standard eeg test that records your brain's electrical activity continuously for a full day, typically while you go about normal life at home. Unlike a routine 20 to 40 minute office EEG, the ambulatory format captures events that might never occur during a short clinic visit, including subtle seizures, sleep-related discharges, and unusual spells. Neurologists rely on this longer window to confirm or rule out epilepsy when a standard EEG comes back normal but symptoms continue.
If you have ever asked what is an eeg test in plain language, the short answer is that it measures tiny voltage changes generated by neurons in your cortex. Sensors called electrodes sit on the scalp, amplifiers boost the signal, and software produces wavy traces that a neurologist reads. A 24 hour eeg uses the same physics but with a small portable recorder you wear in a pouch, allowing the test to follow you through meals, work, exercise, and sleep without keeping you tethered to a hospital bed.
Doctors order ambulatory EEGs for many reasons: unexplained blackouts, possible nocturnal seizures, medication adjustments, suspected non-epileptic events, and follow-up after a normal in-office study. Because seizures are often rare and brief, capturing one during a 30 minute appointment is partly a matter of luck. Stretching the recording across 24 hours dramatically increases the chance of catching abnormal activity, and including a full sleep cycle is especially valuable because many epileptiform patterns appear most clearly during drowsiness and non-REM sleep.
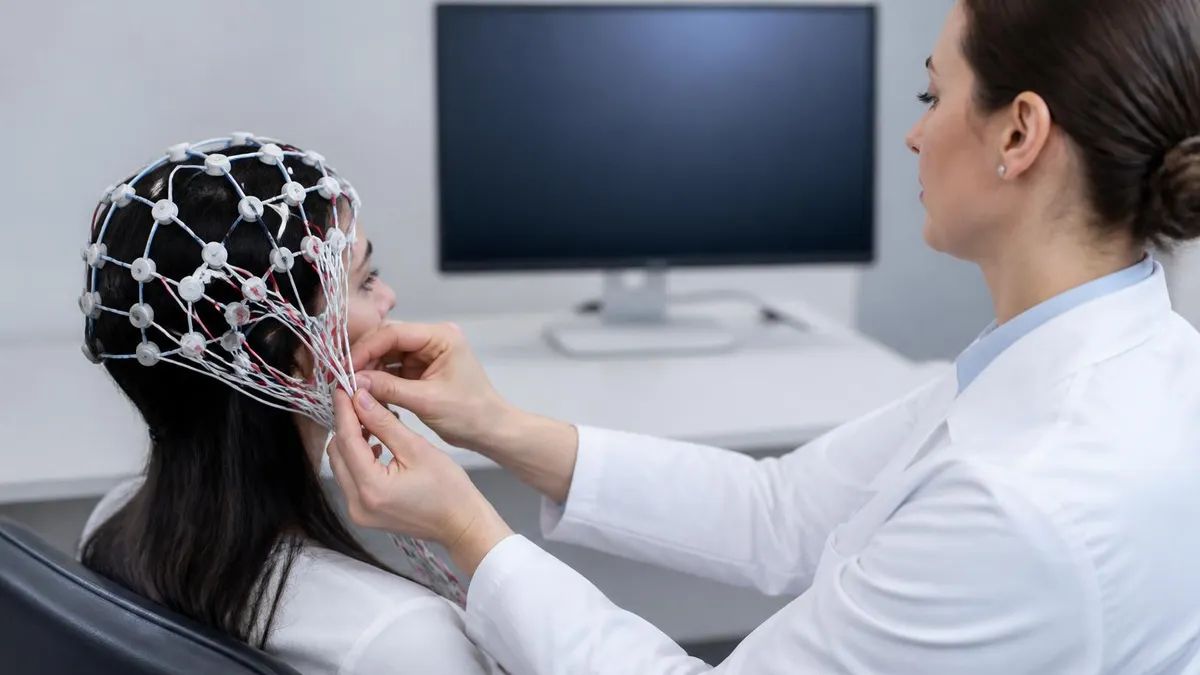
The setup itself is straightforward. A technologist measures your head, marks electrode positions using the international 10-20 system, cleans each spot, and glues small disc electrodes to your scalp with collodion or paste. Wires bundle into a recorder about the size of a paperback book. You leave the clinic with a diary, push-button event marker, and instructions to behave normally. The eeg test side effects are minimal — mostly skin irritation and sticky hair — and you can read more about exactly what the device is picking up below.
Cost varies widely in the US. With insurance, out-of-pocket charges often land between $200 and $800 after deductible, while uninsured cash prices range from roughly $900 to $3,500 depending on hospital versus outpatient facility, video add-on, and length of recording. Many neurology clinics list price transparency information on their websites, and asking specifically about CPT codes 95950 (24 hour EEG) or 95951 (with video) helps you compare apples to apples before scheduling.
Results usually take three to ten business days. A board-certified neurologist or epileptologist reviews the entire recording, marks events you flagged in your diary, and writes a report describing background rhythm, sleep architecture, and any focal or generalized abnormalities. This guide walks through every part of the process — preparation, electrode setup, what is and is not allowed during the recording, interpreting the report, billing strategies, and what to do next if findings come back abnormal, borderline, or completely normal.
24 Hour EEG by the Numbers
How a 24 Hour EEG Works Step by Step
Scheduling and Pre-Test Instructions
Electrode Application
Recorder Hookup and Testing
24 Hours at Home
Return and Removal
Neurologist Review and Report
Doctors order a 24 hour eeg when shorter recordings have failed to answer a clinical question or when the events of concern are too infrequent for a routine study to catch. The most common indication is suspected epilepsy with a normal or inconclusive 30 minute EEG. Roughly half of people with epilepsy show normal interictal recordings on a single short study, so extending the window to a full day raises the diagnostic yield significantly without committing to inpatient video monitoring.
Another frequent reason is differentiating epileptic seizures from non-epileptic events such as syncope, panic attacks, parasomnias, or psychogenic non-epileptic spells. Each of these conditions has a very different treatment path, and getting it wrong can mean years on the wrong medications. Recording during a real-world event — captured because the patient is wearing the device when it happens — provides objective evidence that a clinic-only study cannot match. The how long is an eeg test question matters here: more time means more chances.
Sleep is the third major driver. Many epileptic patterns appear preferentially during light sleep, deep sleep, or the transition between sleep stages. A patient who cannot fall asleep on demand in a noisy clinic chair may sleep deeply at home, exposing abnormalities that were hidden during a brief in-office nap attempt. Frontal lobe and benign rolandic seizures, in particular, often only show up during sleep, making the ambulatory format especially useful for children and young adults with nocturnal events.
Medication management is another use case. When a neurologist adjusts antiepileptic drugs, follow-up ambulatory EEGs document whether epileptiform discharges have decreased, increased, or simply shifted. Insurance plans sometimes require this objective evidence before approving newer medications. Similarly, before weaning a patient off seizure medication after years of control, many epileptologists order a 24 to 72 hour study to confirm that subclinical activity has not returned during waking or sleep.
Cognitive complaints, unexplained falls, and transient confusional spells in older adults round out the indication list. Temporal lobe seizures in seniors often present as memory blanks or staring spells rather than dramatic convulsions, and they're easy to miss on a half-hour recording. A 24 hour eeg can pick up the characteristic temporal lobe discharges and clarify whether dementia, vascular disease, or focal epilepsy is the underlying driver. The same logic applies to suspected absence seizures in school-aged children who keep zoning out in class.
Finally, post-stroke patients, traumatic brain injury survivors, and patients in early dementia evaluations sometimes get ambulatory EEGs to characterize background slowing, asymmetries, or epileptiform abnormalities that would not appear on routine testing. While these uses are less common, they show how flexible the test is. The bottom line: when symptoms point to a brain electrical problem and a short EEG has not delivered answers, a 24 hour study is usually the next logical step before considering inpatient long-term monitoring.
EEG Practice Test Questions
Prepare for the EEG - Electroencephalography exam with our free practice test modules. Each quiz covers key topics to help you pass on your first try.
EEG Abnormal Epileptiform Patterns
EEG Exam Questions covering Abnormal Epileptiform Patterns. Master EEG Test concepts for certification prep.
EEG Activation Procedures
Free EEG Practice Test featuring Activation Procedures. Improve your EEG Exam score with mock test prep.
EEG Artifact Identification
EEG Test Prep for Artifact Identification. Practice EEG Quiz questions and boost your score.
EEG Electrode Placement and Montages
EEG Questions and Answers on Electrode Placement and Montages. Free EEG practice for exam readiness.
EEG - Electroencephalography Abnormal Epil...
EEG Mock Test covering - Electroencephalography Abnormal Epileptiform Patterns. Online EEG Test practice with instant feedback.
EEG - Electroencephalography Activation Pr...
Free EEG Quiz on - Electroencephalography Activation Procedures. EEG Exam prep questions with detailed explanations.
EEG - Electroencephalography Artifact Iden...
EEG Practice Questions for - Electroencephalography Artifact Identification. Build confidence for your EEG certification exam.
EEG - Electroencephalography Electrode Pla...
EEG Test Online for - Electroencephalography Electrode Placement and Montages. Free practice with instant results and feedback.
EEG - Electroencephalography Instrumentati...
EEG Study Material on - Electroencephalography Instrumentation and Calibration. Prepare effectively with real exam-style questions.
EEG - Electroencephalography Neuroanatomy ...
Free EEG Test covering - Electroencephalography Neuroanatomy and Physiology. Practice and track your EEG exam readiness.
EEG - Electroencephalography Non-Epileptif...
EEG Exam Questions covering - Electroencephalography Non-Epileptiform Abnormalities. Master EEG Test concepts for certification prep.
EEG - Electroencephalography Normal EEG Wa...
Free EEG Practice Test featuring - Electroencephalography Normal EEG Waveforms. Improve your EEG Exam score with mock test prep.
EEG - Electroencephalography Patient Safet...
EEG Mock Exam on - Electroencephalography Patient Safety and Ethics. EEG Study Guide questions to pass on your first try.
EEG - Electroencephalography Pediatric and...
EEG Test Prep for - Electroencephalography Pediatric and Neonatal EEG. Practice EEG Quiz questions and boost your score.
EEG ICU and Continuous EEG Monitoring
EEG Questions and Answers on ICU and Continuous EEG Monitoring. Free EEG practice for exam readiness.
EEG Instrumentation and Calibration
EEG Mock Test covering Instrumentation and Calibration. Online EEG Test practice with instant feedback.
EEG Neuroanatomy and Physiology
Free EEG Quiz on Neuroanatomy and Physiology. EEG Exam prep questions with detailed explanations.
EEG Non-Epileptiform Abnormalities
EEG Practice Questions for Non-Epileptiform Abnormalities. Build confidence for your EEG certification exam.
EEG Normal EEG Waveforms
EEG Test Online for Normal EEG Waveforms. Free practice with instant results and feedback.
EEG Patient Safety and Ethics
EEG Study Material on Patient Safety and Ethics. Prepare effectively with real exam-style questions.
EEG Test Price and Insurance Coverage
With commercial insurance, a 24 hour EEG is usually covered when ordered for a documented medical reason like suspected epilepsy or unexplained spells. Your share depends on deductible status, copay structure, and whether the lab is in-network. Most patients pay between $200 and $800 out of pocket after insurance applies discounts.
Medicare reimburses CPT 95950 at roughly $300 to $450 for the technical and professional components combined. Medicare Advantage plans may require prior authorization. Always ask the clinic to verify your benefits and quote the patient-responsibility estimate in writing before scheduling so you are not surprised by a balance bill later.
24 Hour EEG vs Routine In-Office EEG
- +Records 24+ hours instead of 20 to 40 minutes, dramatically increasing seizure capture
- +Patient sleeps in their own bed, often producing clearer sleep stages
- +Captures events triggered by real-world activities like work stress or exercise
- +Includes a full sleep cycle when many epileptiform patterns emerge
- +Less expensive than inpatient video-EEG monitoring or epilepsy unit admission
- +Lets neurologists correlate symptoms in your diary with electrical activity
- −Setup takes 45 to 90 minutes versus about 20 for a routine EEG
- −Cannot shower, swim, or wash hair during the 24 hour recording
- −Electrode glue can irritate skin and is messy to remove
- −Cash price is 3 to 5 times higher than a standard EEG
- −No real-time video unless you upgrade to ambulatory video-EEG
- −Wires can come loose during sleep, requiring a clinic visit to reattach
EEG Test Preparation Checklist
- ✓Wash your hair the morning of setup with regular shampoo only — no conditioner, oils, or hairspray
- ✓Avoid braids, extensions, hair gel, mousse, or any styling product on the day of the test
- ✓Eat a normal breakfast unless your neurologist specifically tells you to fast
- ✓Bring a list of current medications including doses and timing for the tech to record
- ✓Wear a loose button-down or zip-front shirt so you don't pull wires over your head
- ✓Pack a soft beanie or scarf to wear over the wires for the 24 hour period if desired
- ✓Bring a notebook and pen for the activity and symptom diary, even if the clinic supplies one
- ✓Arrange a ride if you suspect a seizure could happen during the drive home
- ✓Keep your phone charged — you may need it to log events or contact the clinic
- ✓Plan to sleep in your usual bed at your usual time to capture realistic sleep architecture
Keep a detailed event diary
The single biggest factor in a useful 24 hour EEG report is the activity and symptom diary. Write down meals, naps, medications, exercise, and any unusual feeling — even a fleeting déjà vu — with the exact clock time. Neurologists match those timestamps to the recording to determine whether spells are electrical events or something else.
Understanding your 24 hour eeg report takes a little vocabulary. The report opens with a technical summary describing recording quality, montage used, length, and whether activation procedures like hyperventilation or photic stimulation were performed. Most ambulatory studies skip activation procedures because the goal is naturalistic recording, but some clinics include a brief hyperventilation block at hookup. If you see references to artifact, that usually means non-brain signals — muscle, eye movement, sweat, or electrode pop — that the reader noted and filtered out.
Next comes the background description. Awake background should show a posterior dominant rhythm in the alpha range (8 to 13 Hz) that reactively blocks when you open your eyes. The reader will comment on symmetry, frequency, and amplitude. Sleep is described stage by stage: drowsiness with theta slowing, stage N2 with spindles and K-complexes, stage N3 with high-amplitude delta, and REM with rapid eye movements and low-amplitude mixed frequencies. A normal report says the background and sleep architecture were within normal limits.
The findings section is where abnormalities live. Words like spikes, sharp waves, polyspikes, spike-and-slow-wave complexes, and generalized spike-and-wave indicate epileptiform activity. Focal slowing — for example left temporal theta — points to a regional brain dysfunction without necessarily meaning seizures. Periodic patterns like PLEDs or GPEDs are seen in acutely ill patients but rarely in routine outpatient ambulatory studies. The neurologist labels each finding by location, frequency, and clinical correlation with your diary entries.
An electrographic seizure section appears if the recording captured actual ictal activity. The reader describes onset location, evolution, spread pattern, and duration, then notes whether you pressed the event button or logged a symptom at that time. A captured seizure with matching diary entry is the gold standard — it tells your neurologist exactly which brain region is responsible and which seizure type you have, guiding medication selection precisely.
Finally, the impression and recommendations summarize everything in plain language. Common impressions include normal awake and asleep EEG, mildly abnormal due to focal slowing, abnormal due to interictal epileptiform discharges, or abnormal with electrographic seizures. Recommendations may suggest starting or adjusting medication, ordering MRI, repeating the ambulatory study with video, or proceeding to inpatient epilepsy monitoring. Always ask your neurologist to walk you through the impression line by line during the follow-up visit.
A normal report does not always rule out epilepsy. Roughly 10 percent of people with confirmed epilepsy have repeatedly normal ambulatory recordings because their seizures are deep, infrequent, or arise from regions scalp electrodes cannot reach. If symptoms persist after a normal 24 hour study, the next steps usually include a longer recording, video correlation, MRI with epilepsy protocol, or referral to a level 4 epilepsy center for inpatient evaluation. Persistent symptoms with negative testing is a clinical scenario, not a closed case.
Pediatric reports follow the same format but emphasize age-appropriate background. Children show different posterior dominant rhythm frequencies depending on age, and benign variants like 14-and-6 positive spikes or wickets are common and not pathologic. A skilled pediatric neurologist will explicitly note these as normal variants so parents do not panic. If you see any term you do not recognize, write it down and ask at follow-up — there are no dumb questions when your brain is the topic.
Some clinics ask you to taper antiepileptic drugs before a 24 hour EEG to increase seizure capture, but only do this if your neurologist specifically instructs it. Stopping medication abruptly on your own can trigger dangerous prolonged seizures or status epilepticus. Always confirm medication instructions in writing before changing anything.
Side effects from a 24 hour eeg are generally mild and limited to the skin and hair. The most common complaint is scalp irritation where electrodes were glued, especially in people with sensitive skin. The collodion adhesive is acetone-based and can cause redness, itching, or mild burning during removal. Patients with eczema, psoriasis, or recent scalp dermatitis should mention this beforehand so the tech can use gentler adhesives like paste or skin-friendly tape alternatives where possible.
Hair-related side effects are predictable. Expect sticky residue and clumping at electrode sites that takes two or three shampoo cycles to fully wash out. Detangling is easier with a leave-in conditioner after the test, but never before. Patients with long, thick, or coily hair may want to plan a salon visit a day or two after the test. Patients with braided or locked hair styles should call the clinic in advance to discuss electrode placement strategies that avoid disturbing protective styles when possible. The full eeg test price rarely covers post-test hair care.
Sleep disturbance is a real but minor concern. Sleeping with 21 wires and a recorder strapped to your shoulder takes some adjustment, and many patients report lighter sleep on the recording night. This is usually not a problem clinically because even partial sleep often reveals diagnostic information, but if you have severe insomnia or sleep apnea, mention it ahead of time. Some clinics will time the study to start in the early afternoon so the recording captures both wakefulness and a near-normal sleep period.
Safety risks during the recording are very low. There is no radiation, no injection, no contrast, and no anesthesia. The recorder is battery-powered and isolated, so there is no risk of electrical shock. Patients can take all regular medications, drive (in most states with seizure-free status), work at a desk job, and do light exercise. Avoid heavy sweating because perspiration can short out electrodes and create artifact that reduces interpretive quality of the recording.
What you cannot do: shower, swim, soak in a hot tub, use a sauna, or stand in heavy rain. Any submersion or saturation will damage the recorder or pop electrodes off the scalp. Sponge baths below the neck are fine. You should also avoid strong electromagnetic environments — MRI machines obviously, but also high-voltage power equipment, certain industrial settings, and arc welders. These can introduce massive artifact that obscures real brain activity.
Children and elderly patients tolerate the test well with simple modifications. For kids, parents are coached to distract during electrode setup with tablets or favorite shows, and soft headwraps help keep curious fingers off the wires. For older adults, fall risk is the main concern because the recorder pouch can shift balance slightly. A walker or cane user should practice walking with the device before going home. Caregivers should be in the home overnight to handle any nighttime events safely.
Finally, allergic reactions to electrode gel or adhesive are rare but possible. Mild redness usually fades within 24 hours of removal. Persistent rash, blistering, or significant swelling warrants a call to the clinic or your primary care provider. True allergic contact dermatitis is uncommon, but documenting any reaction helps the lab choose different materials if you need a repeat study or follow-up monitoring in the future.
Practical tips can turn a frustrating 24 hour eeg into a smooth experience that actually answers your clinical question. Start by treating the day before the test like a sleep hygiene reset: limit caffeine after lunch, avoid alcohol entirely, and go to bed at your usual time. A well-rested patient produces cleaner recordings and is less likely to fall asleep during the hookup, which can prolong setup. If your neurologist requests sleep deprivation, follow the exact hours specified — too little sleep is dangerous, too much defeats the purpose.
Dress strategically. Choose a button-down or zip-front shirt, comfortable pants without metal hardware near the recorder pouch, and slip-on shoes. Bring a second outfit in your bag in case you spill food or coffee — you cannot easily change clothes that pull over your head with wires attached. A scarf, beanie, or stretchy headband over the electrodes adds a polished look if you need to go to work or run errands during the recording.
Plan your 24 hours intentionally. The goal is normal life, but normal life with attention. Eat at your usual times, take medications on schedule, do your routine activities, and write everything down. If you typically experience spells during specific triggers — flickering lights, stress at work, exercise, certain foods — try to include those in the recording window. If you have never had a spell while sitting still, do not just sit still for 24 hours; that wastes the study's diagnostic potential.
Use the event button liberally. Pressing it does not delete data or interrupt the recording — it simply drops a digital bookmark that the neurologist will review carefully. Press for any unusual feeling: lightheadedness, déjà vu, sudden anxiety, a strange smell, brief confusion, twitching, or staring spells you notice. Even false alarms are useful because they help the reader rule events in or out. Under-reporting is the much bigger mistake.
Keep the recorder dry and protected. The pouch usually clips to a belt or hangs on a shoulder strap. At night, place it on a bedside table or tuck it next to your pillow so wires do not tug when you roll over. If a wire comes loose, do not panic — call the clinic. Many will guide you through a quick reattachment over the phone, and a few will send a tech to your home if a major electrode falls off entirely.
After the study, take care of yourself. Hair washing takes patience — use baby shampoo or a clarifying shampoo and warm water, work in small sections, and avoid pulling. A wide-tooth comb helps. Acetone wipes from the clinic remove residual collodion but can dry the scalp; follow with a moisturizing conditioner or oil after removal is complete. Most patients are back to normal hair within two days, and the next day you can finally return to all normal activities including swimming and showers.
Lastly, advocate for yourself at the follow-up appointment. Bring a written list of questions: What did the recording show? Was sleep architecture normal? Were there epileptiform discharges, and if so where? Does this confirm or rule out epilepsy? What are the next steps? Ask for a copy of the full report and the raw recording on a USB drive — many neurologists will provide both on request, and having your own copy is valuable if you ever seek a second opinion at an epilepsy center.
EEG Questions and Answers

EEG for Seizures: How the Test Diagnoses Epilepsy and What to Expect

EEG Tech Salary 2026: Pay by State, Experience, and Certification

EEG Images: A Visual Guide to Brain Wave Patterns, Recordings, and Test Results

What Does an EEG Measure? Brain Waves, Electrical Activity, and What Your Results Reveal
EEG Tech Jobs in 2026: Career Paths, Salaries, and How to Get Hired
About the Author
Educational Psychologist & Academic Test Preparation Expert
Columbia University Teachers CollegeDr. Lisa Patel holds a Doctorate in Education from Columbia University Teachers College and has spent 17 years researching standardized test design and academic assessment. She has developed preparation programs for SAT, ACT, GRE, LSAT, UCAT, and numerous professional licensing exams, helping students of all backgrounds achieve their target scores.