EEG Test in a Hospital: What to Expect, How It Works, and What Your Results Mean
Learn what an EEG test in a hospital involves, how long it takes, what it costs, and what your results mean. 🧠 Complete patient guide.
An eeg test performed in a hospital setting is one of the most common neurological diagnostic procedures in modern medicine. Whether you have been referred by your primary care physician or are being evaluated in an emergency department, understanding what an eeg hospital visit involves can ease anxiety and help you prepare. The test records electrical activity in the brain using small sensors attached to the scalp, providing physicians with a real-time map of how your brain is functioning at a cellular network level.
The eeg medical test has been in clinical use since the 1930s, and hospital-based laboratories have refined the procedure into a streamlined, painless experience. Unlike imaging studies such as MRI or CT scans, an EEG does not use radiation or magnetic fields. Instead, it simply detects the tiny electrical impulses that neurons generate naturally as they communicate. This makes it safe for virtually all patients, including children, pregnant women, and people with implanted medical devices.
Hospitals perform EEGs for a wide range of clinical indications. The most frequent reason is to evaluate suspected epilepsy or to characterize seizures that a patient has already experienced. Neurologists also order EEGs to assess altered states of consciousness, monitor patients in intensive care units for subclinical seizure activity, investigate sleep disorders, and evaluate the extent of brain injury after cardiac arrest or stroke. In some centers, EEGs are used intraoperatively to guide neurosurgeons performing complex procedures on or near eloquent cortex.
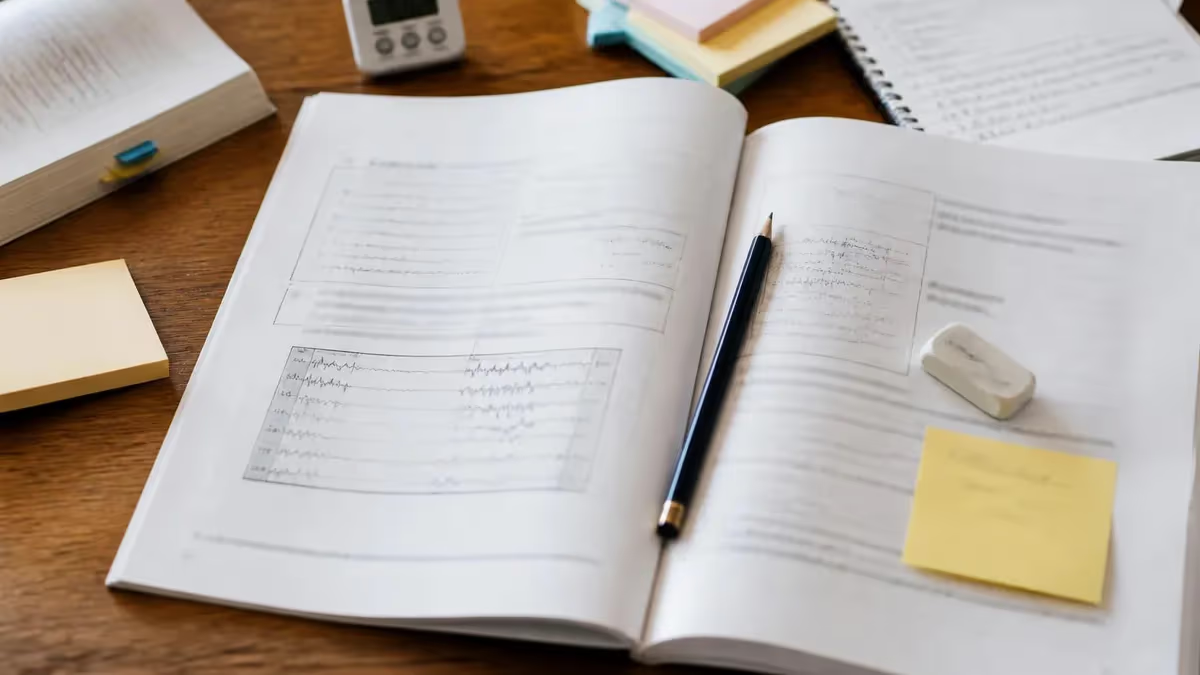
Knowing what is an eeg test before you arrive at the hospital removes much of the mystery. A trained EEG technologist will apply between 19 and 256 electrodes to your scalp using a conductive gel or paste. The electrodes do not inject any electricity — they only record. You will be asked to relax in a reclining chair or on a bed while the technologist captures a baseline recording, typically lasting 20 to 40 minutes for a routine outpatient study. The raw data feeds into an amplifier and then into specialized software that displays waveform traces on a monitor.
During the recording, the technologist may ask you to breathe rapidly for several minutes, a technique called hyperventilation, which can provoke certain abnormal patterns. Photic stimulation — a strobe light flashed at varying frequencies — is another standard activation procedure used to unmask photosensitive epilepsy. Both activations are brief, and the technologist will stop immediately if you experience any discomfort. For patients who require longer monitoring, hospitals offer ambulatory or video-EEG options that can capture days or even weeks of continuous brain activity.
The question of eeg test price and cost concerns many patients. In the United States, a routine hospital-based EEG typically costs between $200 and $900 before insurance adjustments. Prolonged video-EEG monitoring in an epilepsy monitoring unit can run considerably higher, sometimes exceeding $5,000 for multi-day admissions. Most major insurers cover EEGs when ordered for medically necessary indications, but patients should verify their specific benefits and any prior authorization requirements before scheduling. You can also review our dedicated guide on eeg test hospital preparation resources to build familiarity with the procedure before your visit.
Understanding the basics of the EEG helps patients become active participants in their own neurological care. The more informed you are about why the test is ordered, what happens during the recording session, and how results are interpreted, the better equipped you will be to ask meaningful questions and engage in shared decision-making with your care team. This guide walks through every stage of the hospital EEG process, from scheduling your appointment to receiving a final interpretation from the neurologist.
Hospital EEG by the Numbers
Step-by-Step: What Happens During a Hospital EEG
Check-In and Intake
Scalp Preparation and Electrode Placement
Baseline Recording
Activation Procedures
Electrode Removal and Cleanup
Neurologist Interpretation and Report
One of the most common questions patients ask before scheduling is how long is an eeg test from arrival to discharge. For a standard routine outpatient EEG, plan to spend approximately 60 to 90 minutes at the hospital or clinic. Electrode application alone takes 20 to 30 minutes because the technologist must carefully measure placement sites and achieve low skin impedance at each location. The actual recording portion lasts 20 to 40 minutes, followed by cleanup and any post-procedure instructions. Waiting for preliminary results adds additional time in some settings.
Longer study types require significantly more time and sometimes an inpatient admission. A sleep-deprived EEG, which is frequently ordered when a routine study is inconclusive, asks you to stay awake for all or most of the night before the appointment. You arrive at the lab already fatigued, which makes it much easier for the technologist to capture the slow-wave and sleep-onset patterns that most reliably provoke interictal epileptiform discharges. These studies typically run 60 to 90 minutes of recording time but can extend further if the patient takes an unusually long time to fall asleep in the lab environment.
Video-EEG monitoring in an epilepsy monitoring unit is at the opposite end of the spectrum in terms of duration. Patients are admitted to a specialized hospital unit where continuous EEG recording is combined with synchronized video surveillance. The goal is to capture one or more habitual seizures or episodes so that the clinical event can be correlated directly with the brainwave pattern occurring at that moment.
Monitoring periods typically range from 3 to 7 days, though some patients require up to 2 weeks before a diagnostic event is recorded. During the admission, anti-seizure medications may be carefully tapered to increase seizure likelihood — a medically supervised process performed only in settings equipped for immediate intervention.
Ambulatory EEG offers a middle ground in duration and setting. The technologist applies a lightweight portable recorder that you take home and wear continuously for 24 to 72 hours. You return the device at the end of the recording period and go about your normal daily routine in the meantime, pressing an event button whenever you notice a symptom.
The portability is ideal for patients whose events are infrequent and unlikely to occur during a brief lab visit. To learn more about this monitoring modality, see our article on eeg hospital and overnight brain wave testing, which covers how extended studies are interpreted and what typical findings look like.
Neonatal and pediatric EEGs introduce additional duration considerations. Infants are often recorded during natural sleep, which means the technologist may need to time the study around feeding schedules to ensure the baby is drowsy when the cap is applied. Older children who are anxious or uncooperative may require a mild oral sedative prescribed by the neurologist, which adds time for the sedation to take effect and for monitoring during recovery. Pediatric EEG labs are specifically designed to minimize stress, with child-friendly decor, distraction toys, and technologists trained in developmental communication.
Intraoperative EEG and electrocorticography (ECoG) are specialized hospital procedures performed in the operating room. The duration is dictated entirely by the surgical procedure itself, which may last 4 to 12 hours. Intraoperative neurophysiology monitoring technologists and neurophysiologists work alongside the surgical team, watching for changes in background rhythms that could signal impending ischemia or cortical injury. This real-time feedback allows the neurosurgeon to adjust the operative approach before a permanent deficit occurs, making continuous EEG monitoring a critical safety tool during resections near the motor strip, speech areas, or hippocampus.
Intensive care unit EEG monitoring represents yet another duration category. Critically ill patients in neuro-ICUs are frequently monitored for 24 to 72 continuous hours to detect nonconvulsive status epilepticus, a dangerous condition in which the brain experiences continuous seizure activity without obvious outward convulsions. Without EEG, this diagnosis is easily missed, and delays in treatment are associated with significantly worse neurological outcomes. Continuous ICU monitoring requires bedside EEG equipment, dedicated amplifiers, and software capable of generating compressed spectral array displays that nurses can interpret at a glance between formal neurologist reviews.
What Is an EEG Medical Test Used to Diagnose?
Epilepsy diagnosis is the single most common indication for an EEG test in hospital and outpatient settings alike. Neurologists look for interictal epileptiform discharges — spikes, sharp waves, and spike-and-slow-wave complexes — that indicate a brain region has an increased tendency to generate abnormal synchronous firing. The location of these discharges helps classify the epilepsy syndrome and guides medication selection. Focal discharges suggest a lesional or structural cause, while generalized 3-Hz spike-and-wave bursts point toward genetic generalized epilepsy syndromes such as juvenile absence epilepsy or juvenile myoclonic epilepsy.
It is important for patients to understand that a normal EEG does not rule out epilepsy. Only about 50 percent of people with confirmed epilepsy show interictal discharges on a first routine EEG. Repeated studies, sleep-deprived recordings, and prolonged ambulatory monitoring substantially increase the diagnostic yield. Conversely, approximately 2 percent of the general population without epilepsy shows incidental epileptiform variants, which is why EEG findings must always be interpreted alongside the full clinical picture rather than in isolation.
Hospital EEG vs. Outpatient Clinic EEG: Key Differences
- +Hospital EEG labs offer immediate access to neurologist consultation if an abnormality is detected during recording
- +Full epilepsy monitoring units allow multi-day video-EEG admissions not available in standalone outpatient clinics
- +Hospital-based labs are equipped for neonatal and pediatric EEGs requiring specialized electrode sets and monitoring
- +ICU continuous EEG monitoring is only available in hospital settings with dedicated bedside equipment
- +Emergency EEGs for status epilepticus can be initiated within minutes in a hospital with an on-call technologist
- +Hospital accreditation standards require regular equipment calibration and technologist credentialing quality reviews
- −Hospital EEG test cost is typically higher than an independent outpatient clinic due to facility fees
- −Scheduling wait times at busy academic medical centers can be 2 to 6 weeks for routine studies
- −Parking, navigation, and check-in processes add 30 to 60 minutes to the overall visit in large hospital systems
- −Inpatient insurance billing can be more complex, with separate facility and professional fee components
- −Hospital environments can increase patient anxiety, potentially affecting the quality of the baseline recording
- −Outpatient clinics sometimes offer more flexible appointment times, including early morning or weekend slots
How to Prepare for Your Hospital EEG Test
- ✓Wash your hair the night before with regular shampoo and do not apply any conditioner, gel, spray, or oil on the day of the test.
- ✓Get the amount of sleep your neurologist recommends — some orders specify sleep deprivation to increase diagnostic yield.
- ✓Take all routine medications as prescribed unless your neurologist has explicitly instructed you to hold a specific drug.
- ✓Avoid caffeine for at least 8 hours before the appointment because stimulants can alter background EEG rhythms.
- ✓Bring a complete medication list including doses, frequencies, and the prescribing physician's name.
- ✓Arrive 15 minutes early to complete intake paperwork and allow time for the technologist to review your clinical history.
- ✓Wear comfortable, loose-fitting clothing — you may recline in a chair or lie on a table for up to 40 minutes.
- ✓Inform the technologist of any scalp conditions, skin sensitivities, or recent head trauma before electrode application begins.
- ✓Ask a family member or friend to drive you if your neurologist has restricted driving due to seizure risk.
- ✓Plan to wash your hair again after the study to remove conductive paste — bring a comb or brush if you prefer to tidy up at the hospital.
A Normal EEG Does Not Rule Out Epilepsy
Up to 50 percent of people with confirmed epilepsy have a normal first routine EEG. If your initial study is unremarkable but your symptoms strongly suggest seizures, ask your neurologist about a sleep-deprived study or prolonged ambulatory monitoring — both significantly increase the chance of capturing diagnostic brainwave patterns that a brief awake recording misses entirely.
Understanding what is an eeg test result means requires a basic familiarity with how neurologists categorize brainwave patterns. The primary frequency bands observed in a clinical EEG are delta (0.5–4 Hz), theta (4–8 Hz), alpha (8–13 Hz), and beta (13–30 Hz). In a healthy awake adult, the dominant background activity over the posterior head regions is alpha, which characteristically attenuates or disappears when the eyes are opened — a phenomenon called alpha blocking. The presence of appropriate alpha and beta activity in an awake, cooperative patient is the first thing a neurologist confirms before evaluating for abnormalities.
Abnormal EEG findings fall into two broad categories: epileptiform and non-epileptiform. Epileptiform abnormalities include spikes (transient sharply contoured waveforms lasting 20 to 70 milliseconds), sharp waves (similar morphology but 70 to 200 milliseconds in duration), and spike-and-slow-wave complexes in which each spike is followed by a slow wave. These patterns indicate cortical hyperexcitability and are highly associated with epilepsy, though their presence alone is not diagnostic — they must be correlated with the patient's clinical history, seizure semiology, and neuroimaging findings before a management decision is made.
Non-epileptiform abnormalities include focal or diffuse slowing, which reflects underlying structural or functional disruption of the cortex or white matter. Focal theta or delta slowing over one hemisphere often correlates with a structural lesion visible on MRI such as a tumor, stroke, or area of prior surgery. Diffuse slowing, in which the dominant background frequency is slower than expected for the patient's age and level of alertness, suggests metabolic encephalopathy, medication effect, or global cerebral dysfunction. Recognizing the difference between focal and diffuse patterns is one of the core interpretive skills that EEG readers develop through years of supervised training.
Benign EEG variants are normal patterns that can be misinterpreted as pathological by less experienced readers. Wicket spikes, breach rhythms over skull defects, 14-and-6-Hz positive spikes, and small sharp spikes are among the most commonly misread variants. The American Clinical Neurophysiology Society maintains standardized terminology guidelines specifically to reduce inter-reader variability and prevent over-diagnosis of epilepsy based on normal variants. Patients who are told their EEG showed a spike or sharp wave should ask whether the finding represents a true epileptiform discharge or one of these recognized normal variants.
Specific EEG patterns are closely associated with particular epilepsy syndromes, and recognizing these patterns guides both diagnosis and treatment selection. Hypsarrhythmia — a high-amplitude chaotic pattern of multifocal spikes and slow waves — is the hallmark of infantile spasms (West syndrome) and indicates the need for urgent treatment with ACTH or vigabatrin.
The 3-Hz generalized spike-and-wave pattern during absence seizures is so characteristic that its presence essentially confirms the diagnosis of childhood absence epilepsy. Lennox-Gastaut syndrome is defined in part by slow spike-and-wave (less than 2.5 Hz) and paroxysmal fast activity during sleep, reflecting the severe and refractory nature of this epileptic encephalopathy.
Patients frequently ask about eeg test side effects, and it is reassuring to know that the procedure itself carries virtually no risk of adverse effects. The electrodes do not deliver electrical current, so there is no possibility of shock or tissue injury from the recording electrodes. The conductive gel may cause mild scalp irritation in patients with sensitive skin, but this resolves within hours of removal.
The activation procedures carry slightly more nuance: hyperventilation can provoke absence seizures in susceptible patients, which is actually desirable because it confirms the diagnosis. In extremely rare cases, photic stimulation can trigger a more prolonged seizure in patients with photosensitive epilepsy, which is why the neurologist is notified immediately and the lab maintains emergency protocols.
The final neurologist report will classify the EEG as normal, abnormal with specific descriptors, or indeterminate. An abnormal result does not automatically mean you have epilepsy — it means your brainwave pattern contains features that require clinical correlation. Your neurologist will integrate the EEG findings with your symptom history, neurological examination, and any relevant neuroimaging before making a diagnostic conclusion. In many cases, a single EEG provides enough information to guide initial treatment, while in others a series of studies or prolonged monitoring is needed to arrive at a confident clinical diagnosis.
If you experience a prolonged seizure lasting more than 5 minutes, repeated seizures without full recovery between episodes, or a seizure followed by persistent confusion lasting more than 30 minutes, call 911 immediately. These scenarios may represent status epilepticus, a neurological emergency requiring IV medication and continuous EEG monitoring in a hospital setting — not a routine outpatient EEG appointment.
The question of eeg test cost is one that patients, caregivers, and healthcare administrators all grapple with. In the United States, the technical fee for a routine EEG at a hospital outpatient department ranges from approximately $200 to $900 depending on geographic region, facility type, and payer mix. This technical component covers the equipment, consumables, technologist time, and facility overhead.
A separate professional fee is billed by the interpreting neurologist or clinical neurophysiologist, typically ranging from $75 to $200. Patients with commercial insurance usually owe only a co-payment or the remaining deductible after their plan's negotiated rate is applied, but those with high-deductible plans may bear the full cost until the deductible is met.
Medicare and Medicaid reimbursement rates are lower than commercial insurance rates and vary by CPT code. A routine EEG lasting less than one hour is billed under CPT 95816 for awake and drowsy studies or CPT 95819 for awake and asleep studies. Prolonged EEGs, video-EEG monitoring, and ICU continuous monitoring each carry distinct CPT codes with higher facility and professional fee allowances. Understanding which CPT code your physician plans to use before the study helps you estimate your out-of-pocket responsibility more accurately and allows time to appeal if an insurer initially denies coverage as not medically necessary.
Patients without insurance or those facing coverage denials have several options to reduce their financial exposure. Many hospital systems offer charity care programs that provide free or reduced-cost services to patients whose household income falls below a defined threshold, typically 200 to 400 percent of the federal poverty level. Federally Qualified Health Centers (FQHCs) offer EEG services on a sliding-fee schedule tied to income.
Some academic medical centers have clinical research protocols that include EEG monitoring at no cost to participants who meet eligibility criteria. Negotiating a self-pay discount directly with the hospital billing department before the service is performed can also yield reductions of 20 to 50 percent from the chargemaster rate.
Insurance prior authorization is increasingly required for EEGs, particularly for prolonged or video-EEG monitoring admissions. The ordering neurologist's office typically manages this process, but patients should confirm that authorization was obtained before the scheduled date to avoid unexpected denials. If your insurer denies an EEG request on the grounds that it is not medically necessary, you have the right to request a peer-to-peer review between your neurologist and the insurer's medical director. Published data consistently show that peer-to-peer reviews reverse an initial denial in 50 to 70 percent of cases when the ordering physician presents the clinical rationale in detail.
Hospital billing errors are unfortunately common with EEG claims, and patients are encouraged to request an itemized bill and compare it against the explanation of benefits (EOB) sent by their insurer. Common discrepancies include duplicate charges, billing for a longer study duration than was actually performed, and incorrect facility or professional fee splits.
If you identify a discrepancy, contact the hospital billing department in writing and request a formal review. Keep copies of all correspondence and document every phone call with the date, time, and name of the representative. Persistent billing disputes can be escalated to your state insurance commissioner or a patient advocacy organization.
The eeg test cost landscape is also shaped by where you live. Urban academic medical centers typically have higher facility fees than community hospitals or freestanding neurology clinics, even for identical CPT codes. Telehealth for EEG interpretation has grown significantly since 2020, with some companies offering remote reading services that reduce the professional fee component for rural hospitals that lack on-site clinical neurophysiologists.
Patients in rural areas sometimes travel to larger centers for complex monitoring but can have routine EEGs performed locally and the results transmitted electronically to a remote reader, reducing both travel burden and total cost. For a comprehensive breakdown of national price benchmarks, our dedicated cost guide covers eeg test price variations by state, facility type, and insurance status in detail.
Financial planning for an EEG admission, particularly a multi-day epilepsy monitoring unit stay, should begin well before the scheduled date. Request a cost estimate from the hospital's financial counseling office, which is required to provide good-faith estimates under the No Surprises Act.
Use this estimate to set up a payment plan if needed, explore health savings account (HSA) or flexible spending account (FSA) funds, and apply for any available assistance programs. Being proactive about the financial conversation reduces stress during what is already an anxiety-provoking medical experience and ensures that cost concerns do not cause a patient to delay or cancel a clinically necessary diagnostic procedure.
Preparing effectively for an EEG technologist certification exam requires the same systematic approach that patients benefit from when preparing for an actual hospital EEG test. Whether you are studying for the ABRET R. EEG T. credential or the CLTM, building a strong conceptual foundation in the clinical indications for hospital EEG is essential. Examination questions frequently draw on real-world hospital scenarios: recognizing which patients require continuous ICU monitoring, knowing the appropriate response when a patient seizes during activation procedures, and understanding how to document and communicate critical findings to the clinical team are all high-yield topic areas.
Technologists working in hospital settings must be comfortable with a wider range of clinical situations than their outpatient counterparts. The hospital EEG technologist may be called at 2 AM to set up continuous monitoring on a comatose ICU patient, assist with intraoperative ECoG in the operating room, or record a neonatal EEG on a premature infant in the NICU. Each of these environments has unique electrode application challenges, equipment configurations, and communication protocols. Mastering the technical demands of hospital EEG practice is a significant differentiator for job applicants and contributes meaningfully to patient safety and diagnostic quality.
Documentation skills are particularly critical in the hospital environment. Technologists must accurately record the patient's level of consciousness, any medications received in the hours before the study, the exact times of activation procedures, and any clinical events observed during recording. This contemporaneous documentation becomes part of the permanent medical record and directly informs the neurologist's interpretation. Incomplete or inaccurate annotations — for example, failing to note that a patient fell asleep or was agitated during recording — can lead to misinterpretation of artifacts as pathological patterns or genuine abnormalities as movement artifact.
Artifact recognition is one of the most practically demanding skills in hospital EEG interpretation. The hospital environment introduces numerous sources of electrical interference that are not present in quiet outpatient labs: ventilators, infusion pumps, cardiac monitors, and electrocautery units all generate electrical signals that can contaminate the EEG tracing.
ECG artifact appears as a regular, rhythmic waveform time-locked to the cardiac cycle and can be distinguished from a cortical discharge by comparing its timing with a simultaneously recorded ECG channel. Pulse artifact, caused by electrode movement over a scalp vessel, creates slower rhythmic oscillations that vary with respiration. Experienced technologists learn to recognize and document these artifacts so that the neurologist can confidently exclude them from interpretation.
The regulatory and credentialing landscape for hospital EEG programs has strengthened considerably over the past decade. The Joint Commission and state health departments inspect EEG labs as part of hospital accreditation surveys, reviewing equipment calibration records, technologist credentials, quality assurance data, and report turnaround times. Many hospitals require that EEG technologists hold the ABRET R. EEG T. credential within a defined period of hire and maintain continuing education hours for credential renewal every five years. These standards exist to protect patients from diagnostic errors that could result in inappropriate treatment decisions.
Research and innovation in hospital EEG continues to advance rapidly. Quantitative EEG (qEEG) tools generate automated measures of spectral power, coherence, and asymmetry that supplement visual review and facilitate monitoring by non-neurologist bedside staff. Machine learning algorithms trained on large annotated EEG datasets have demonstrated performance approaching that of expert readers in detecting seizures and classifying seizure types, and several FDA-cleared devices are now available for clinical use in seizure detection.
High-density EEG arrays with 64 to 256 channels, combined with source localization software, allow researchers and epileptologists to reconstruct the three-dimensional generators of scalp-recorded activity with unprecedented spatial resolution, enhancing pre-surgical evaluation for drug-resistant epilepsy.
The future of hospital EEG lies in integration with the broader neurological monitoring ecosystem. Combining EEG with near-infrared spectroscopy, transcranial Doppler, intracranial pressure monitoring, and continuous biomarker measurement creates a multimodal picture of brain health that no single modality can provide alone. Hospitals investing in neuroinformatics platforms that aggregate and display these signals in a unified dashboard are positioning themselves to deliver a new standard of neurocritical care that is proactive rather than reactive, detecting deterioration before it becomes clinically apparent and enabling earlier, more targeted interventions across the spectrum of acute brain injury.
EEG Questions and Answers

EEG Electroencephalography Practice Test PDF (Free Printable 2026)

Sleep EEG: How Overnight Brain Wave Testing Works and What Your Results Mean

EEG Test Cost in 2026: Prices, Insurance Coverage, and How to Save

Travel EEG Tech Jobs: The Complete Guide to Working as a Mobile Electroencephalography Technologist

EEG Pronunciation, Meaning, and Everything You Need to Know About the EEG Test
About the Author
Educational Psychologist & Academic Test Preparation Expert
Columbia University Teachers CollegeDr. Lisa Patel holds a Doctorate in Education from Columbia University Teachers College and has spent 17 years researching standardized test design and academic assessment. She has developed preparation programs for SAT, ACT, GRE, LSAT, UCAT, and numerous professional licensing exams, helping students of all backgrounds achieve their target scores.