Define Functional MRI: How fMRI Works, What It Measures, and Why It Matters
Define functional MRI in plain English. Learn how fMRI measures brain activity, BOLD signals, clinical uses & limits. 🧠 Complete 2026 June guide.

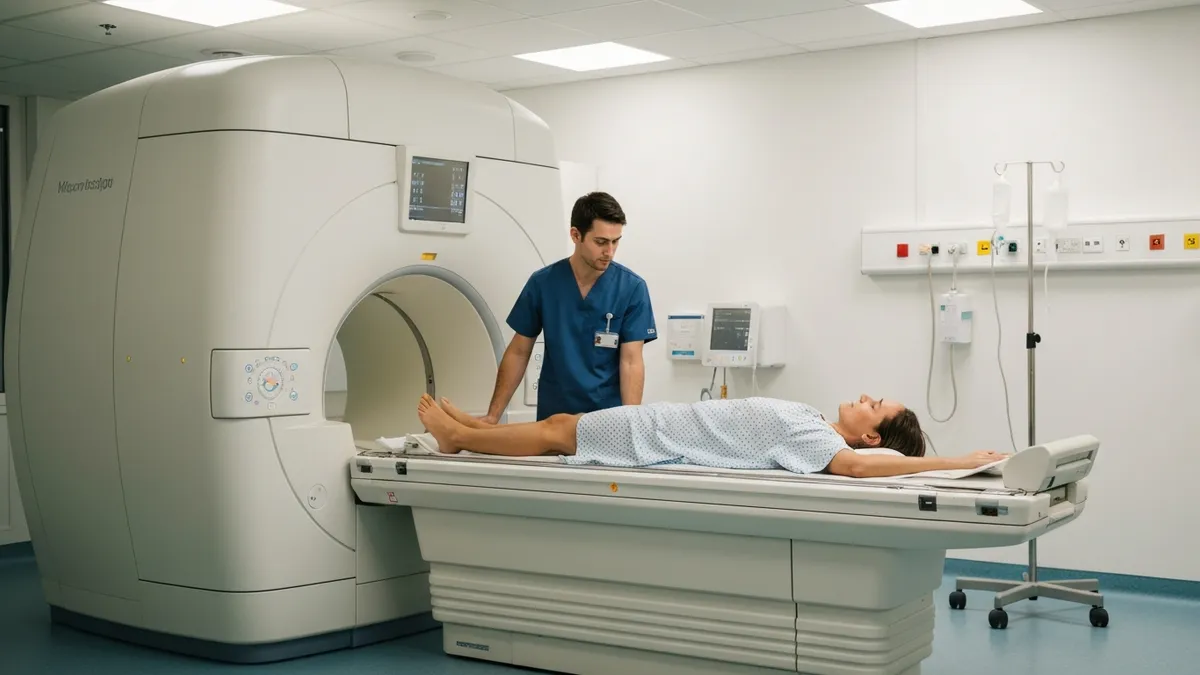
To define functional MRI precisely: functional magnetic resonance imaging, universally abbreviated as fMRI, is a neuroimaging technique that detects real-time changes in blood oxygenation across the brain to infer where and when neural activity is occurring. Unlike conventional structural MRI, which produces static anatomical pictures, fMRI generates dynamic maps that reveal which brain regions become more or less active in response to a specific task, stimulus, or resting state. Understanding how to define functional MRI is foundational for radiologists, neuroscientists, and MRI technologists alike.
The physiological principle underlying fMRI is elegantly simple: neurons that fire consume oxygen, and the vascular system responds by delivering a surge of freshly oxygenated blood to the active area within one to five seconds. Because oxygenated hemoglobin and deoxygenated hemoglobin have different magnetic properties, a standard MRI scanner can detect this contrast without any injected dye or radioactive tracer. This contrast mechanism is called the Blood Oxygen Level-Dependent signal, almost always referred to by its acronym BOLD. The BOLD signal is the cornerstone of modern fMRI research and clinical presurgical planning.
fMRI was first demonstrated as a viable imaging method in the early 1990s, when researchers at Bell Labs and Massachusetts General Hospital independently showed that visual stimulation produced detectable BOLD changes in human occipital cortex. Since then, the technique has expanded from a research curiosity into a clinical tool used in more than a thousand hospitals worldwide. It now guides neurosurgeons before brain tumor resections, helps map language and motor function in epilepsy patients, and provides objective biomarkers in psychiatric research trials studying conditions from depression to schizophrenia.
From a technical standpoint, fMRI requires a high-field MRI scanner, typically 1.5 Tesla or 3 Tesla in clinical settings, and uses echo-planar imaging sequences that can acquire whole-brain volumes every one to two seconds. This rapid acquisition rate allows researchers to track the slow hemodynamic response that follows neural firing. Modern 7 Tesla research scanners push spatial resolution below one millimeter, revealing the columnar and laminar architecture of the cortex that was previously visible only in post-mortem histology specimens.
The data produced by a single fMRI session can be enormous. A typical thirty-minute scan generates several gigabytes of raw image data, and the preprocessing and statistical analysis pipeline involves multiple correction steps including motion correction, slice-timing correction, spatial smoothing, and registration to a standard brain atlas. Software packages such as FSL, SPM, and AFNI have become essential companions to the scanner hardware, transforming raw signal fluctuations into color-coded statistical maps that clinicians and researchers can interpret at a glance.
fMRI has proven especially valuable as a complement to functional mri definition methods like diffusion-weighted imaging, which traces white-matter fiber pathways between brain regions. Together, BOLD-based fMRI and diffusion tractography give clinicians both the functional hotspots and the structural highways connecting them, a combination that is transforming pre-operative neurosurgical planning and deepening our understanding of network-level brain disorders such as Alzheimer disease and autism spectrum disorder.
This guide covers everything you need to know about fMRI: the physics of the BOLD signal, the hardware requirements, clinical indications, how task-based and resting-state paradigms differ, the strengths and limitations of the technique, and how fMRI knowledge appears on MRI registry and board examinations. Whether you are a student preparing for certification or a clinician looking to sharpen your understanding, the sections below provide a thorough and accurate foundation.
Functional MRI by the Numbers

How the BOLD Signal Works: Step by Step
Neural Firing Begins
Neurovascular Coupling
BOLD Signal Rises
Hemodynamic Response Function
Statistical Mapping
Clinical or Research Output
When clinicians and researchers talk about fMRI paradigms, they distinguish between two broad categories: task-based fMRI and resting-state fMRI. Task-based fMRI is the older and more clinically mature approach. The patient or research participant performs a structured behavioral protocol inside the scanner — tapping fingers, reading words silently, listening to tones, or following visual instructions — while the scanner acquires rapid whole-brain BOLD images. Brain regions that show a statistically significant increase in BOLD signal during the task condition compared to a rest or control condition are inferred to be involved in performing that task.
The design of the task protocol matters enormously for data quality. Block designs, in which the participant alternates between long epochs of task and rest lasting fifteen to thirty seconds each, produce the strongest and most reliable BOLD signals because the hemodynamic response accumulates across many repeated stimuli within each block. Event-related designs, by contrast, present individual stimuli or trials separated by variable inter-trial intervals and are better suited to isolating responses to specific event types or to paradigms where blocking is not cognitively appropriate, such as fear conditioning or oddball detection studies.
Resting-state fMRI, introduced in the mid-1990s by Biswal and colleagues, asks participants to lie still with eyes open or closed and simply let their minds wander. No task is performed. Yet even in this resting condition, the BOLD signal fluctuates spontaneously in patterns that are highly reproducible across individuals. Brain regions that show correlated spontaneous fluctuations are said to belong to the same resting-state network, and researchers have identified a reproducible set of seven to seventeen such networks in the healthy human brain, including the default mode network, the salience network, and sensorimotor networks corresponding to each body part.
The default mode network — encompassing the medial prefrontal cortex, posterior cingulate cortex, and lateral parietal regions — is perhaps the most studied resting-state network. It is consistently deactivated during demanding external tasks and activated during self-referential thought, autobiographical memory retrieval, and future planning. Disruption of the default mode network has been reported in Alzheimer disease, schizophrenia, major depressive disorder, and attention deficit hyperactivity disorder, making it a promising biomarker target for clinical trials evaluating new psychiatric and neurological treatments.
Independent component analysis (ICA) is the statistical method most commonly used to decompose resting-state fMRI data into its constituent networks without requiring a pre-specified model. ICA separates the total variance in the BOLD time series into spatially independent components, some of which correspond to genuine neural networks and others to artifacts such as head motion, cardiac pulsation, and respiratory cycles. Dual regression extends single-subject ICA maps to group comparisons, enabling researchers to test whether patients with a neurological disease show weaker or stronger connectivity within a given network compared to healthy controls.
Motion artifacts represent the single biggest confound in both task-based and resting-state fMRI. Even sub-millimeter head movements during scanning can induce BOLD signal changes that mimic genuine neural responses or spuriously inflate functional connectivity estimates. Standard preprocessing pipelines apply rigid-body motion correction, but recent research has shown that even after this step, residual motion-related signal persists and must be removed using scrubbing — the exclusion of time points with framewise displacement exceeding 0.2 to 0.5 millimeters — or using ICA-based noise classifiers such as ICA-FIX or AROMA.
For MRI certification candidates, understanding the distinction between task-based and resting-state fMRI, and knowing that both rely on the BOLD signal and neurovascular coupling, is essential exam knowledge. Questions may also test familiarity with the hemodynamic response function shape, the typical TR range used in fMRI sequences, and the field strengths commonly employed in clinical versus research settings. Practicing with free registry-style questions is the most effective way to consolidate this conceptual knowledge into reliable exam performance.
Clinical Applications of Functional MRI
The most established clinical use of fMRI is pre-surgical cortical mapping in patients with brain tumors, arteriovenous malformations, or drug-resistant epilepsy. Before the advent of fMRI, neurosurgeons relied on intraoperative cortical stimulation — the Wada test or awake craniotomy — to identify eloquent cortex. These procedures carry procedural risks and patient discomfort. Non-invasive fMRI mapping, performed days or weeks before surgery, allows the surgical team to plan the safest possible resection trajectory based on the spatial relationship between the lesion and functional hotspots for motor control, language production, and language comprehension.
Typical pre-surgical fMRI protocols include finger-tapping and hand-squeezing tasks to map primary motor cortex; word-generation and sentence-listening tasks to lateralize and localize Broca's and Wernicke's areas; and visual checkerboard stimulation to confirm occipital lobe integrity. The language lateralization index derived from fMRI — calculated as the asymmetry of activation between left and right hemispheres — has shown 90–95% concordance with the traditional Wada test in large multicenter studies, leading many epilepsy programs to reduce or eliminate routine Wada testing in favor of fMRI alone.

Advantages and Limitations of fMRI
- +Non-invasive and radiation-free — safe for repeated scanning in research and pediatric populations
- +Whole-brain coverage in a single acquisition with sub-second temporal sampling
- +High spatial resolution compared to EEG and MEG — localizes function to within 2–3 millimeters clinically
- +No injected contrast agent required — BOLD signal is intrinsic to blood oxygenation
- +Validates language lateralization without invasive Wada testing in presurgical patients
- +Enables resting-state network mapping even in non-responsive or sedated patients
- −BOLD signal is indirect — measures blood flow changes, not neural activity itself
- −Poor temporal resolution compared to EEG — hemodynamic lag of 4–6 seconds obscures rapid neural dynamics
- −Highly sensitive to patient motion — even millimeter-level movement degrades data quality significantly
- −Signal dropout near air-tissue interfaces (sinuses, ear canals) causes blind spots in orbitofrontal and temporal pole regions
- −Requires statistical thresholding — threshold choice affects which activations appear, creating researcher degrees of freedom
- −7 Tesla systems achieve highest resolution but are expensive and not widely available outside research centers
fMRI Exam Prep Checklist for MRI Registry Candidates
- ✓Define the BOLD signal and explain why deoxygenated hemoglobin is paramagnetic while oxygenated hemoglobin is diamagnetic.
- ✓Describe neurovascular coupling and identify the cell types (neurons, astrocytes, pericytes) involved in triggering arteriolar dilation.
- ✓Explain the shape of the hemodynamic response function including the initial dip, peak overshoot, and post-stimulus undershoot.
- ✓Compare block designs and event-related designs — know when each is used and their relative statistical power.
- ✓Identify the typical repetition time (TR) range used in fMRI echo-planar sequences (1–3 seconds for whole-brain coverage).
- ✓State the minimum clinical field strength for fMRI (1.5 Tesla) and explain why 3 Tesla is preferred for presurgical mapping.
- ✓Describe at least three clinical indications for fMRI including presurgical motor mapping, language lateralization, and tumor planning.
- ✓List three major resting-state networks: default mode, salience, and sensorimotor, and their main component brain regions.
- ✓Explain why head motion is the largest confound in fMRI and name two mitigation strategies (motion correction, scrubbing).
- ✓Identify signal dropout artifact locations in fMRI (orbitofrontal cortex and temporal poles near air-tissue interfaces) and their cause.
The BOLD Signal Is Indirect — and That Is Always on the Exam
A question that consistently appears on MRI registry and board examinations asks what the BOLD signal actually measures. The correct answer is that it measures the ratio of oxygenated to deoxygenated hemoglobin, which reflects changes in cerebral blood flow — not neural electrical activity directly. Candidates who confuse BOLD with direct electrophysiological recording consistently lose these points. Solidify this distinction early and revisit it in your practice questions.
Understanding the limitations of fMRI is just as important as appreciating its strengths, particularly for clinicians who must counsel patients and interpret reports accurately. The most fundamental limitation is that BOLD is an indirect measure of neural activity. It captures vascular changes driven by neurovascular coupling, and any condition that disrupts this coupling — cerebrovascular disease, medications that alter vascular tone, carbon dioxide level fluctuations from hyperventilation or breath-holding — can produce misleading results.
In patients with gliomas, the tumor's own aberrant vasculature may not couple normally, potentially causing fMRI to underestimate the true extent of functional involvement and leading surgeons to plan overly aggressive resections near eloquent cortex.
The spatial resolution of clinical fMRI, while impressive by neuroscience standards at two to three millimeters isotropic, is still macroscopic. Individual cortical columns responsible for a specific finger movement or phoneme representation span only a few hundred micrometers. Clinical fMRI maps a region, not the precise functional architecture within it.
This means that when the nearest active voxel is one centimeter from the tumor edge, a cautious surgeon cannot be certain the true functional boundary does not extend slightly closer. Intraoperative electrocortical stimulation remains the gold standard for identifying the precise surgical limit, with preoperative fMRI serving as a guide to prioritize stimulation sites rather than a definitive boundary marker.
Temporal resolution is fMRI's other major limitation relative to electrophysiological methods. Neural computations in the cortex unfold on millisecond timescales, but the BOLD hemodynamic response peaks four to six seconds after the triggering neural event. This temporal blurring makes it impossible to use fMRI alone to determine the sequence of brain areas activated during a complex cognitive task. Researchers often pair fMRI with EEG (high temporal resolution, poor spatial resolution) in a multimodal design that leverages the complementary strengths of both modalities to reconstruct both where and when neural processing occurs with much greater precision than either technique alone.
Statistical analysis choices also introduce significant variability into fMRI results. The choice of statistical threshold, the spatial smoothing kernel size, the motion regression strategy, and the software package used can all shift activation maps meaningfully. A landmark 2020 study by Botvinik-Neeman and colleagues demonstrated that seventy different analysis teams, each analyzing the same fMRI dataset, produced substantially different activation maps and reached different scientific conclusions. This analytical flexibility — sometimes called the garden of forking paths — underscores the importance of pre-registration in fMRI research and careful protocol standardization in clinical imaging programs.
Field inhomogeneity is a physics-level limitation that creates signal dropout in specific brain regions. At air-tissue interfaces — the frontal sinuses just above the orbitofrontal cortex and the petrous bones adjacent to the temporal poles — local magnetic field gradients created by the susceptibility difference between air and tissue cause rapid T2* dephasing. BOLD signal in these regions is severely diminished or absent. Parallel imaging techniques, z-shimming, and multi-echo acquisition strategies can partially recover signal in these regions, but clinicians and researchers must always note that orbital frontal and anterior temporal lobe findings may be incomplete due to this artifact.
Scanner noise is an underappreciated practical challenge in auditory fMRI paradigms. Echo-planar imaging sequences generate acoustic noise exceeding 100 decibels, which activates auditory cortex continuously during scanning. Sparse-sampling and clustered-volume acquisition protocols address this by acquiring brain volumes in brief bursts with long silent gaps, allowing researchers to present auditory stimuli in the quiet intervals and then measure the BOLD response during the subsequent acquisition. Without such adaptations, the scanner noise itself overwhelms the auditory cortex response to any experimental stimulus.
For MRI technologists and registry candidates, familiarity with these limitations is clinically relevant because they affect scan protocol choices, patient preparation instructions, and the appropriate framing of fMRI results in reports and consultations. Knowing that a patient with extensive sinus disease will have orbitofrontal dropout, or that a patient on a vasodilating medication may show altered BOLD coupling, directly informs the quality and interpretability of the scan acquired — and separates a knowledgeable technologist from one who simply runs the protocol without understanding its underlying assumptions.
Presurgical fMRI maps are planning tools, not intraoperative boundaries. Neurosurgeons should always combine fMRI results with intraoperative electrocortical stimulation mapping before resecting tissue within two centimeters of an activated region. fMRI false-negative rates in tumor patients can reach 10–15% due to neurovascular uncoupling, meaning absent activation does not guarantee absent function. Never assume a region is safe to resect based solely on the absence of fMRI signal.
For MRI technologists preparing for ARRT or ARMRIT registry examinations, fMRI is a high-yield topic that bridges physics, physiology, and clinical application — exactly the combination that examination writers favor. Questions may ask you to identify the correct echo time for BOLD imaging (typically 30–40 milliseconds at 3 Tesla, chosen to maximize T2* contrast), the reason EPI is used instead of conventional gradient echo sequences (speed — EPI can acquire a full slice in tens of milliseconds versus seconds), or the role of the shimming process in optimizing field homogeneity before an fMRI session begins.
Patient preparation for clinical fMRI differs meaningfully from routine brain MRI preparation. Patients must be able to perform the required tasks reliably inside the scanner, which means screening for cognitive deficits, language barriers, hearing impairment, and claustrophobia before the appointment. The technologist must explain each task paradigm clearly and verify that the patient can perform it correctly during a practice run outside the scanner. A patient who misunderstands the finger-tapping task or falls asleep during the resting-state acquisition produces unusable data, wasting scanner time and potentially delaying a critical surgical decision.
Head motion restriction is the most important practical concern during fMRI acquisition. Technologists should use foam padding to minimize head movement within the coil, provide clear instructions to remain still, and monitor motion parameters in real time if the acquisition software permits.
Some centers use a bite bar or a custom-molded mouthguard to further restrict motion in cooperative patients, particularly those undergoing high-field research scans where sub-millimeter motion correction thresholds apply. Pediatric patients and patients with movement disorders present the greatest challenge and may require light sedation, though sedation itself alters neurovascular coupling and must be noted in the scan report.
From a sequence perspective, technologists should understand that fMRI uses T2*-weighted gradient echo EPI, not the T2-weighted spin echo sequences used in conventional brain MRI or the diffusion-sensitized sequences used in DWI. The gradient echo EPI sequence is exquisitely sensitive to local field inhomogeneities — which is precisely what makes it sensitive to BOLD changes — but this same sensitivity makes it prone to geometric distortions near air-tissue interfaces. Field map correction, acquired as part of the standard fMRI protocol in most modern implementations, measures the actual field inhomogeneity distribution and applies a voxel-by-voxel geometric distortion correction during preprocessing.
Parallel imaging acceleration, using techniques such as GRAPPA or SENSE, is routinely applied in fMRI to reduce the echo train length of EPI readouts and thereby decrease geometric distortion and signal dropout. Simultaneous multi-slice (SMS) imaging, also called multiband EPI, accelerates whole-brain acquisition by exciting and sampling multiple slices simultaneously using radiofrequency pulses with multiple frequency components and controlled controlled aliasing reconstruction. SMS factors of two to eight are now standard in research fMRI protocols, allowing whole-brain coverage with 2-millimeter isotropic voxels in under 600 milliseconds — a dramatic improvement over the 2–3 second TRs common a decade ago.
When reviewing fMRI reports as a clinician or technologist, it is important to scrutinize the statistical threshold and cluster extent used to define activations. Reports that do not specify these parameters should be interpreted with caution, as overly liberal thresholds can produce spurious activations in regions not truly engaged by the task.
The commonly used threshold of p less than 0.001 uncorrected was shown in a widely publicized 2016 paper by Eklund and colleagues to produce false-positive rates as high as 70% in some software implementations when cluster-extent thresholding is used — a finding that prompted major revisions to default analysis settings in all major fMRI software packages and reinforced the importance of family-wise error or false discovery rate correction for clinical reports.
As the field evolves toward faster acquisition, higher field strengths, and more sophisticated analysis methods including deep learning-based denoising and automated network parcellation, the role of the informed MRI technologist becomes more important rather than less. A technologist who understands the physics of BOLD, the goals of the paradigm, and the confounds that can corrupt the data is a critical member of the clinical fMRI team — one who can troubleshoot acquisition issues in real time and ensure that each patient's scan provides the neurologist and neurosurgeon with the highest-quality functional map possible.
Looking ahead, several emerging directions in fMRI promise to expand its clinical and research utility substantially. Ultra-high-field MRI at 7 Tesla and beyond offers dramatically improved BOLD sensitivity and spatial resolution, enabling layer-specific and column-specific functional mapping that was previously impossible in living human subjects. Laminar fMRI, which resolves BOLD responses across the six cortical layers with sub-millimeter voxels, is revealing the directionality of information flow in cortical circuits — distinguishing feedforward sensory signals arriving in layer 4 from feedback signals arriving in layers 1–2, a distinction with profound implications for understanding consciousness, attention, and predictive coding.
Accelerated fMRI using simultaneous multi-slice acquisition has enabled large-scale precision functional mapping studies in which individual participants complete ten or more hours of scanning across multiple sessions, producing individual brain connectivity profiles with the same reliability as fingerprints. These precision connectome maps reveal highly reproducible individual differences in functional network organization that predict cognitive abilities, educational attainment, and risk for mental health disorders — differences that are completely washed out when data from many individuals are simply averaged together in conventional group studies.
Naturalistic fMRI paradigms present participants with rich, continuous stimuli such as films, podcasts, and social interactions rather than simple laboratory tasks, enabling the study of complex social cognition and narrative comprehension in conditions that more closely approximate everyday life. Inter-subject correlation analysis, which measures the degree to which different participants show synchronized BOLD responses while watching the same film, has revealed that brain regions involved in social understanding and narrative processing become tightly synchronized across individuals during engaging stories — and that this synchronization is reduced in autism spectrum disorder and social anxiety disorder.
Machine learning and artificial intelligence are transforming fMRI analysis in both research and clinical contexts. Convolutional neural networks trained on large fMRI datasets can classify brain states — sleeping versus awake, resting versus task-engaged, healthy versus diseased — with accuracies that rival or exceed traditional statistical approaches. Decoder models trained on visual cortex BOLD patterns can reconstruct the image a participant was viewing from brain activity alone, a capability with obvious implications for brain-computer interface development for paralyzed individuals who cannot speak or move but whose visual cortex remains intact.
The integration of fMRI with other neuroimaging modalities continues to deepen. PET-MRI hybrid scanners now allow simultaneous measurement of BOLD and neuroreceptor availability, glucose metabolism, or amyloid plaque burden — combining the functional sensitivity of fMRI with the molecular specificity of radioligand PET in a single imaging session. This combination is particularly powerful in Alzheimer disease research, where amyloid deposition detectable by PET appears to disrupt default mode network connectivity measurable by fMRI years before any cognitive symptoms emerge, potentially enabling intervention at a stage when disease-modifying treatments may still be effective.
For students and clinicians approaching fMRI for the first time, the conceptual framework is more accessible than the technical complexity might suggest. The core logic is straightforward: active neurons need more oxygen, the blood supply overresponds by delivering a surplus of oxygenated hemoglobin, and the MRI scanner detects the resulting change in local magnetic properties. Everything else — the acquisition sequences, the preprocessing pipelines, the statistical models, and the interpretation frameworks — is an elaboration of this foundational relationship between neural activity and blood flow that makes fMRI the uniquely powerful window into the living human brain it has become.
Whether you are studying for an MRI registry examination, preparing to assist with presurgical fMRI cases in a clinical setting, or simply trying to understand the neuroimaging literature you encounter in continuing education, mastering the definition, mechanism, and applications of functional MRI positions you at the frontier of one of medicine's most dynamic and impactful imaging technologies. The investment in understanding fMRI thoroughly repays itself many times over in clinical competence, examination performance, and the ability to contribute meaningfully to a field that is reshaping our understanding of the human brain.
MRI Questions and Answers

DWI MRI: Diffusion-Weighted Imaging Explained (2026 Guide)
Side Effects of Brain MRI: Understanding Risks, Safety, and What Every Patient Should Know
MRI Lumbar Spine Without Contrast: Complete Guide to the Scan, What It Shows, and How to Prepare

MRI History: From Nuclear Resonance to Modern Scanners

MRI of Cervical Spine: Complete Guide to Imaging, Anatomy, Pathology, and Patient Preparation
About the Author
Medical Laboratory Scientist & Clinical Certification Expert
Johns Hopkins UniversityDr. Sandra Kim holds a PhD in Clinical Laboratory Science from Johns Hopkins University and is certified as a Medical Technologist (MT) and Medical Laboratory Scientist (MLS) through ASCP. With 16 years of clinical laboratory experience spanning hematology, microbiology, and molecular diagnostics, she prepares candidates for ASCP board exams, MLT, MLS, and specialist certification tests.
Join the Discussion
Connect with other students preparing for this exam. Share tips, ask questions, and get advice from people who have been there.
View discussion (4 replies)