Montreal Cognitive Assessment Practice Test: Complete Guide to MoCA Questions
Master montreal cognitive assessment questions with free practice tests, scoring guides, and expert tips. 🎯 Start your MoCA prep today.

Montreal cognitive assessment questions are the cornerstone of one of the most widely used screening tools in modern medicine. The MoCA — short for Montreal Cognitive Assessment — is a 30-point test administered by clinicians to detect mild cognitive impairment, early Alzheimer's disease, and other forms of dementia.
Whether you are a patient preparing for an upcoming appointment, a family caregiver trying to understand what to expect, or a healthcare student studying cognitive screening, knowing how these questions work puts you far ahead of the curve. Understanding the structure and purpose of each domain gives you genuine confidence walking into any clinical encounter.
The MoCA was developed by Dr. Ziad Nasreddine in Montreal, Canada, and published in 2005. Since then it has become a gold standard for rapid cognitive screening, used in clinics, hospitals, and research settings across more than 55 countries. Unlike the older mmse test, the MoCA was specifically designed to catch subtle deficits that more basic tools miss. It evaluates eight distinct cognitive domains within a single 10-to-15-minute administration window, making it remarkably efficient for busy clinical environments without sacrificing diagnostic sensitivity.
One of the most frequently searched topics in cognitive health is how the MoCA compares to something like the mini mental status exam (MMSE). Both tools measure cognitive function, but the MoCA is broadly considered more sensitive for detecting mild cognitive impairment — the stage between normal aging and dementia. Patients who score in the normal range on the MMSE sometimes still show deficits on the MoCA, which is why neurologists and geriatric specialists increasingly prefer it. Knowing which tool your provider will use helps you prepare more purposefully and understand the significance of your score.
Preparing for the MoCA is not about memorizing answers — the questions are different each time, and clinicians are trained to avoid predictable prompting. Instead, meaningful preparation involves understanding what each domain measures, practicing similar cognitive tasks regularly, and maintaining the lifestyle habits that support brain health. Think of MoCA preparation like training for an athletic event: you build underlying fitness rather than rehearse a specific script. Regular mental exercise, quality sleep, cardiovascular activity, and social engagement all contribute to peak cognitive performance on test day.
High-profile cases have brought the MoCA into mainstream awareness. Public figures including former President Donald Trump and President Biden have discussed cognitive screening publicly, sparking widespread interest in what a trump cognitive decline discussion actually reveals about the test's clinical validity. When politicians or celebrities mention their MoCA scores, it underscores how the assessment has moved from niche clinical practice into broad public consciousness. This heightened visibility means more people are seeking practice resources, explanations of the domains, and honest guidance about what scores actually mean — exactly what this guide provides.
This article walks you through every domain of the MoCA, explains the types of montreal cognitive assessment questions you can expect, offers strategies for each section, and provides links to free practice quizzes you can use right now. Whether your goal is self-education, caregiver preparation, clinical study, or personal peace of mind, this resource gives you everything you need to approach the MoCA with knowledge and confidence. We will cover the visuospatial section, memory tasks, attention exercises, language prompts, abstraction questions, and the naming and orientation components in clear, practical detail.
Beyond test mechanics, we also address the emotional context of cognitive screening. Many people feel anxious about taking the MoCA, worried about what results might mean for their independence or health trajectory. That anxiety is completely normal and understandable.
The goal of screening is early detection — catching changes while there is still maximum opportunity to intervene, adjust medications, recommend lifestyle changes, or connect patients with memory care specialists. An imperfect score is not a sentence; it is information, and information empowers better decisions. Approaching the MoCA with that mindset transforms it from a source of fear into a useful health tool.
Montreal Cognitive Assessment by the Numbers
MoCA Exam Format: Domains, Points, and Time
| Section | Questions | Time | Weight | Notes |
|---|---|---|---|---|
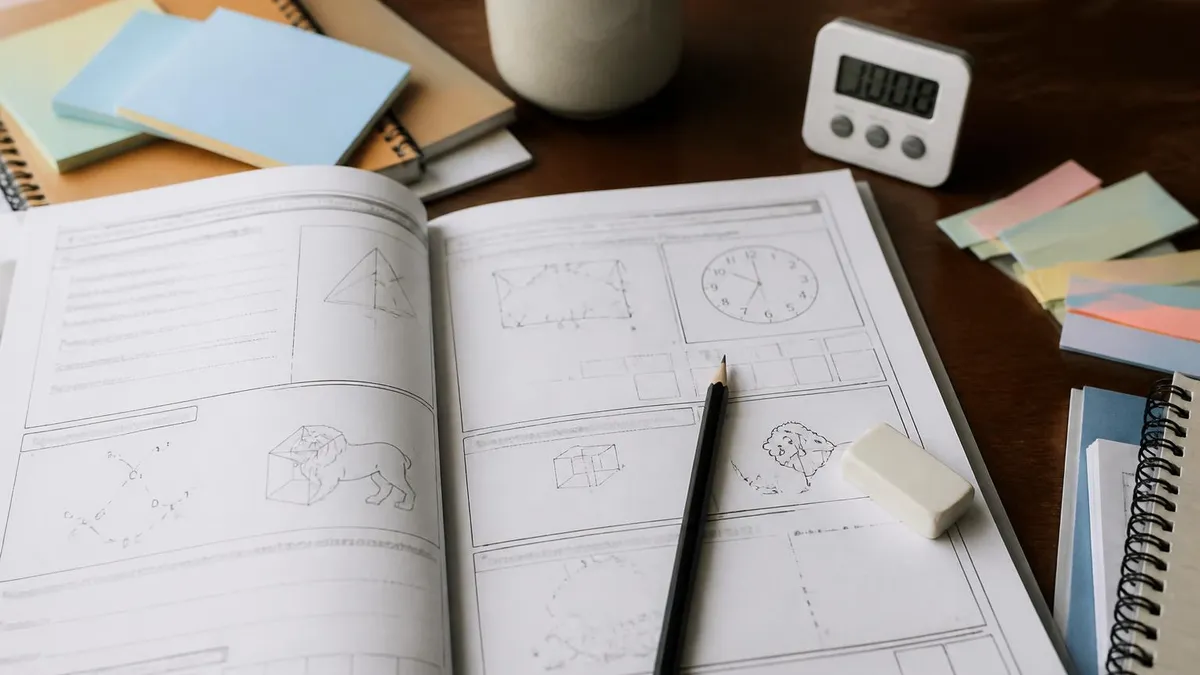
| Visuospatial / Executive | 5 | 2–3 min | 17% | Trail-making, cube copy, clock draw |
| Naming | 3 | 1 min | 10% | Identify 3 animals from drawings |
| Memory (Delayed Recall) | 5 | 3–4 min | 17% | Recall 5 words after delay |
| Attention & Concentration | 6 | 2–3 min | 20% | Digit spans, serial 7s, vigilance |
| Language | 3 | 1–2 min | 10% | Repeat sentences, fluency task |
| Abstraction | 2 | 1 min | 7% | Similarity pairs (e.g., train/bicycle) |
| Orientation | 6 | 1 min | 20% | Date, month, year, day, place, city |
| Total | 30 | 10–15 minutes | 100% |
Understanding how montreal cognitive assessment questions are structured is essential preparation for anyone who will undergo or administer the test. The MoCA follows a standardized paper-and-pencil format, though digital versions are increasingly available. A trained administrator — typically a physician, nurse practitioner, neuropsychologist, or trained technician — guides the patient through each section in a fixed sequence. The entire assessment fits on a single double-sided page, and all materials needed are provided by the examiner. Patients do not need to bring anything, study materials, or reference documents of any kind.
The visuospatial and executive section opens the MoCA and challenges several higher-order functions simultaneously. The trail-making task asks patients to alternate between numbers and letters in sequence (1-A-2-B-3-C and so on), which tests cognitive flexibility and working memory. The cube-copying task assesses three-dimensional spatial reasoning and fine motor coordination.
The clock-drawing exercise — perhaps the most well-known cognitive screening task — asks patients to draw a clock face, place all 12 numbers correctly, and set the hands to a specified time such as 10 minutes past 11. Errors in clock drawing can reveal deficits in planning, spatial organization, and executive function simultaneously.
The naming section is brief but diagnostically informative. The examiner shows the patient three line drawings of animals — typically a lion, a rhinoceros, and a camel — and asks for identification. These particular animals are chosen because they are universally recognizable yet require specific vocabulary retrieval. A person with early semantic memory loss may struggle to name the rhinoceros even if they clearly recognize it as an animal. This task taps into the temporal lobe's role in storing categorical knowledge and retrieving specific labels under mild time pressure, which makes it a surprisingly sensitive indicator of subtle language deficits.
The memory section involves two presentations of five words — typically FACE, VELVET, CHURCH, DAISY, and RED — followed by immediate recall attempts. Crucially, these words are not scored during the learning trials; only the delayed recall at the end of the MoCA contributes to the score. This design mirrors how real-world memory actually works: we constantly encode information but only retrieve it when needed later. The five-word list is carefully chosen to span different semantic categories (body part, texture, building, flower, color), which prevents clustering strategies from inflating scores and keeps the measure ecologically valid.
Attention and concentration is the domain where many patients are surprised by the difficulty. The forward digit span (repeat 2-1-8-5-4) and backward digit span (repeat 7-4-2 in reverse) test working memory and mental manipulation. The vigilance task requires patients to tap the table every time they hear the letter A read aloud from a long sequence — a sustained attention test.
Serial 7 subtraction (counting backward from 100 by sevens: 93, 86, 79, 72, 65) tests calculation ability under mild cognitive load. Together these tasks probe the prefrontal cortex and parietal networks that support focused, effortful mental work. You can also explore a comprehensive cognitive functions test breakdown to understand domain interactions more deeply.
Language tasks on the MoCA cover two distinct abilities. First, the patient must repeat two syntactically complex sentences verbatim: one is a long declarative sentence and one contains a relative clause structure. Even small omissions or substitutions count as errors. Second, the patient must name as many words as possible beginning with the letter F within 60 seconds. Normal performance is 11 or more words. This phonemic fluency task is sensitive to frontal lobe dysfunction and provides a window into verbal generativity — the ability to rapidly search and retrieve words from memory according to a phonological rule.
Abstraction and orientation round out the MoCA. The abstraction task presents two word pairs — such as train and bicycle, or watch and ruler — and asks how they are similar. Acceptable answers capture the categorical relationship (both are vehicles; both are measuring instruments) rather than surface features. This task tests conceptual reasoning, a higher-order function that degrades early in frontotemporal dementia and in certain stages of Alzheimer's disease.
The orientation section closes the assessment with six questions about the current date, month, year, day of the week, current location, and city. Disorientation to time is often one of the earliest signs of significant cognitive decline, making this section both simple and clinically revealing.
Studying Each MoCA Domain: Mini Mental Health Status Examination vs. MoCA
The delayed recall section is worth five points and is the single highest-value domain on the MoCA. To prepare, practice encoding five unrelated words from different categories and testing yourself after a 5-to-10-minute delay filled with other mental tasks. Use elaborative encoding — create a vivid mental image or story linking each word to the next. Research consistently shows that people who use active encoding strategies retain significantly more information than those who passively read or repeat words. Daily practice with word lists builds both encoding speed and retrieval reliability over time.
Many patients find the memory section most anxiety-inducing because forgetting feels concrete and alarming. It helps to remember that the MoCA memory task measures a very specific type of recall under artificial conditions — not general life competence. Factors like sleep deprivation, medication side effects, depression, anxiety, and even dehydration can temporarily suppress performance. If you score below expectations on practice tests, discuss these variables with your clinician before attributing the result to pathological cognitive decline. A single score in isolation is never a diagnosis; it is one data point in a broader clinical picture.
MoCA vs. Other Cognitive Screens: Benefits and Limitations
- +Higher sensitivity for mild cognitive impairment than the MMSE (90% vs. 18%)
- +Covers eight distinct cognitive domains in a single 10-to-15-minute session
- +Available in 46+ languages, enabling equitable screening across diverse populations
- +Free to use for clinicians and researchers with training certification
- +Widely validated in peer-reviewed research across multiple clinical populations
- +Digital and telephone versions now available for remote or telehealth administration
- −Education level significantly affects scores — low education may produce false positives
- −Anxiety and test-taking nerves can temporarily suppress performance on the day
- −Cultural and language differences can affect naming task and fluency task results
- −One score cannot diagnose dementia — requires broader clinical evaluation to interpret
- −Clock-drawing scoring can vary slightly between different trained administrators
- −Not designed to differentiate between specific dementia subtypes without additional testing
MoCA Prep Checklist: 10 Steps Before Your Assessment
- ✓Get at least 7–8 hours of quality sleep the night before your MoCA appointment.
- ✓Stay well-hydrated on the day of the test — even mild dehydration affects cognition.
- ✓Practice serial 7 subtraction (100, 93, 86, 79, 72, 65) daily for two weeks before testing.
- ✓Memorize the alternating trail-making pattern: 1-A-2-B-3-C-4-D-5-E.
- ✓Rehearse drawing a clock face showing 10 minutes past 11 — practice spatial placement of numbers.
- ✓Practice recalling five unrelated words after a 10-minute delay filled with other tasks.
- ✓Review today's date, month, year, day of the week, and current location the morning of the test.
- ✓Tell your clinician about any medications that might affect cognition or sleep before the test.
- ✓Manage anxiety with a 5-minute breathing exercise immediately before the appointment.
- ✓Complete at least one full MoCA practice quiz to familiarize yourself with the pacing and question flow.
One Point Added for 12 or Fewer Years of Education
The official MoCA scoring protocol automatically adds one point to the total score for any patient who has 12 or fewer years of formal education. This adjustment exists because lower educational attainment can suppress MoCA performance independently of true cognitive status. If you completed less than a full high school education, your adjusted score may qualify as normal even if the raw total appears below the 26-point threshold. Always confirm this adjustment with your clinician when reviewing results.
Understanding MoCA scoring helps contextualize what montreal cognitive assessment questions are actually measuring and what different scores suggest clinically. The maximum possible score is 30 points, and a score of 26 or higher is generally considered within normal limits for adults with 13 or more years of education.
Scores between 18 and 25 are associated with mild cognitive impairment. Scores between 10 and 17 suggest moderate cognitive impairment. Scores below 10 indicate severe cognitive impairment. However, it is critical to emphasize that a single MoCA score is never used in isolation to make a clinical diagnosis — it is one piece of a much larger diagnostic puzzle.
Several factors beyond actual cognitive status influence MoCA scores, and clinicians are trained to weigh these carefully. Age is relevant because normal cognitive processing speed slows with healthy aging, even without disease. Education, as noted, has a systematic effect that the one-point adjustment partially addresses but does not fully neutralize.
Depression and anxiety are frequent confounders — major depressive disorder can reduce MoCA scores by 3 to 5 points in some patients, mimicking the pattern of mild cognitive impairment. Sleep disorders, thyroid dysfunction, vitamin B12 deficiency, and certain medications — including benzodiazepines, anticholinergics, and some antihistamines — can all temporarily suppress performance.
Serial testing is far more informative than any single administration. When clinicians administer the MoCA every six months or annually, the trajectory of scores reveals whether performance is stable, improving, or declining. A one-time score of 24 might reflect education-adjusted normal performance, residual effects of a recent illness, or the early stages of a progressive condition — context and serial comparison determine which interpretation is most accurate.
This is why patients who score below 26 are often asked to return for follow-up testing rather than immediately referred to specialists, unless the score is significantly low or accompanied by other clinical signs.
The moca assessment process is most powerful when combined with informant reports from family members or caregivers who know the patient well. Clinicians often supplement the MoCA with structured caregiver interviews, asking about changes in daily functioning, navigation ability, medication management, and social behavior.
A patient who scores 27 on the MoCA but whose spouse reports significant recent changes in personality, navigation errors, or trouble managing household finances warrants more investigation than the score alone would suggest. Conversely, a patient who scores 24 but whose family reports no functional changes and who attributes the score to exam anxiety may not need urgent specialist referral.
For patients who want detailed domain-level understanding of their performance, clinicians can break down which specific items were missed and analyze the pattern. For example, failing the memory section, the visuospatial section, and the orientation section simultaneously suggests a profile consistent with Alzheimer's disease. Failing primarily the executive function and attention tasks while preserving memory suggests a different profile, potentially consistent with vascular cognitive impairment or certain psychiatric conditions. Pattern recognition of this kind requires clinical training, but understanding that pattern matters helps patients ask better questions during follow-up appointments.
Research on the MoCA has expanded considerably since its 2005 publication. Studies have validated MoCA sensitivity and specificity across dementia subtypes including Alzheimer's disease, Lewy body dementia, frontotemporal dementia, Parkinson's disease dementia, and vascular dementia. Each subtype tends to produce a characteristic pattern of domain-specific failures, which experienced clinicians can use as a preliminary guide for further neuropsychological testing or neuroimaging. The MoCA has also been validated for use with multiple sclerosis patients, individuals with traumatic brain injury, and populations recovering from stroke, expanding its clinical utility far beyond dementia screening alone.
Patients who are determined to optimize their MoCA performance should focus their preparation energy on the domains that contribute most to the score. Delayed memory (5 points) and orientation (6 points) together account for 37 percent of the total score — making these the highest-leverage domains for preparation. Attention tasks (6 points) add another 20 percent.
This means that targeted practice on word recall, date orientation, and serial subtraction covers more than half the total score and represents the most efficient use of preparation time. Abstract thinking (2 points) contributes least and is often the domain where patients naturally perform well, making it a lower priority for focused practice unless a specific weakness has been identified.
A MoCA score below 26 does not automatically mean you have dementia or Alzheimer's disease. Scores can be affected by anxiety, medications, poor sleep, depression, vitamin deficiencies, and many other reversible factors. Always discuss your results with a qualified clinician who has access to your full medical history, current medications, and information from people who know you well. Self-diagnosing based on a practice test result or a single clinical score is never appropriate.
Effective preparation for montreal cognitive assessment questions goes beyond intellectual knowledge — it requires building the underlying cognitive habits that support strong performance across every domain. Think of the brain like any other organ: it responds to consistent, varied stimulation with structural and functional improvements.
Activities that challenge multiple cognitive systems simultaneously — playing a musical instrument, learning a new language, engaging in strategic board games, or navigating new environments without GPS — are particularly effective at building cognitive reserve, the brain's resilience against decline. Cognitive reserve does not prevent diseases like Alzheimer's, but it delays symptom onset and slows functional decline.
Physical exercise is one of the most evidence-backed interventions for cognitive health, and its effects are directly relevant to MoCA performance. Aerobic exercise increases blood flow to the hippocampus — the brain region most critical for memory consolidation and the area most damaged early in Alzheimer's disease.
Studies show that adults who engage in at least 150 minutes of moderate-intensity aerobic exercise per week have significantly better memory, attention, and executive function scores than sedentary adults of the same age. Walking briskly, cycling, swimming, and dancing all count. The effect is dose-dependent: more consistent exercise produces larger cognitive benefits, with improvements observable on standardized tests within as few as six weeks.
Sleep is the brain's primary maintenance window — during deep sleep, the glymphatic system flushes metabolic waste products including amyloid-beta and tau proteins, the very substances that accumulate abnormally in Alzheimer's disease. Chronic sleep deprivation of even one to two hours per night accumulates amyloid burden faster than fully rested controls, according to research from the National Institutes of Health.
For anyone preparing for a MoCA or concerned about cognitive health more broadly, sleep hygiene is not optional maintenance — it is one of the most powerful tools available. Seven to nine hours of quality sleep nightly, consistent wake times, and minimizing blue light exposure before bed are evidence-based recommendations from the American Academy of Sleep Medicine.
Diet significantly influences cognitive performance as well. The Mediterranean diet and the MIND diet (a hybrid emphasizing brain-protective foods) have both been associated with slower cognitive decline and better performance on assessments like the MoCA. These dietary patterns emphasize leafy green vegetables, berries, nuts, olive oil, fish, and whole grains while limiting red meat, butter, cheese, pastries, and fried foods.
Observational studies suggest that people who follow these diets score 7.5 years younger cognitively than peers with Western dietary patterns. While diet cannot reverse existing damage, it creates an internal environment that supports neuronal health and efficient cognitive processing — exactly the conditions needed for strong test performance.
Social engagement also matters more than most people realize. Social isolation accelerates cognitive decline, while rich, varied social interaction appears to be protective. The mechanism involves multiple systems: social conversation demands language retrieval, attention, memory, and theory of mind simultaneously — essentially an informal, enjoyable form of cognitive cross-training. Volunteering, group classes, book clubs, religious communities, and regular family gatherings all provide the kind of engaged social interaction associated with better long-term cognitive outcomes. For people who live alone or whose social networks have shrunk, finding structured community engagement is a genuine health intervention, not just a lifestyle preference.
For immediate preparation in the days before a MoCA assessment, the most important actions are the most basic: sleep well, eat a real meal before the appointment, arrive with enough time to avoid rushing, and bring a list of all current medications for the clinician to review. Avoid alcohol for at least 48 hours before testing.
Inform the administrator of any recent illness, stressful life events, or changes in medications that might affect your baseline performance. If English is not your first language or you have significant hearing or vision impairment, make sure the administrator knows in advance so accommodations can be arranged. A well-prepared patient and a well-informed clinician together produce the most meaningful and actionable assessment results.
The moca assessment form is publicly available for educational purposes, and reviewing it beforehand gives patients a clear picture of the test layout without the pressure of formal administration. Knowing where the clock-drawing task appears, understanding the trial structure of the memory section, and seeing the actual format of the trail-making component reduces the element of surprise that can derail performance for anxious patients.
Self-education is not cheating — it is responsible preparation that leads to more accurate results, since a patient who is calm and clear-headed because they understand the format will perform closer to their true baseline than one who is confused or frightened by the task structure.
On the day of your MoCA appointment, specific strategies can help you perform your best within each individual section. For the visuospatial tasks, take a moment to look at the full trail-making diagram before drawing your first line — visualizing the complete path before starting reduces errors significantly.
For the cube copy, focus on the three-dimensional depth cues in the original drawing before attempting your own version. For clock drawing, lightly mark the 12, 3, 6, and 9 positions first as anchors before filling in the remaining numbers. This planning step takes only seconds but dramatically improves spatial accuracy for people who would otherwise rush directly into drawing.
For the naming task, if you cannot immediately identify one of the animal drawings, give yourself a few additional seconds before giving up. Memory retrieval under mild time pressure can be improved by using category-narrowing self-prompts: ask yourself where this animal lives, what it eats, and how large it is. These associative cues often unlock the specific label when direct retrieval fails. Most administrators allow a reasonable amount of processing time without pressure, and a brief pause to organize your retrieval strategy is entirely appropriate and clinically accepted behavior, not a sign of impairment.
During the memory encoding trials, use deliberate strategies rather than passive repetition. When the five words are read aloud — typically face, velvet, church, daisy, and red — immediately create a vivid mental scene incorporating all five elements: picture a face wearing red velvet outside a church decorated with daisies.
The more bizarre and specific the image, the more memorable it becomes. This encoding technique, known as the method of loci or visual association, is used by memory champions and cognitive neuroscientists alike. It takes only seconds to apply but can increase delayed recall by two to three words above passive repetition for most adults.
The serial 7 subtraction task is worth pausing to approach strategically. If you make an error midway — say you subtract incorrectly and get 79 instead of 79 — the administrator is typically trained to score only the incorrectly computed steps, not every step that follows.
This means that if you make one arithmetic error but then correctly subtract seven from your wrong answer for the next steps, you still receive credit for those subsequent steps. Knowing this rule reduces the catastrophic feeling of making one mistake and abandoning the rest of the sequence. Keep going after any error and complete all five subtractions regardless of confidence in any individual step.
Orientation questions close the MoCA and are worth six total points — making them simultaneously the most straightforward and highest-value domain on a per-question basis. In the days before your appointment, make a conscious habit of noting the complete date each morning: day of the week, date, month, and year. Know the specific name of the facility or clinic where you will be tested, as well as the city.
If you frequently travel or spend time between multiple locations, confirm in advance which address you should use as your reference for location questions. This simple daily habit ensures that six easy points are locked in rather than lost to momentary disorientation in an unfamiliar clinical environment.
After your MoCA results are available, ask your clinician to walk through each domain with you and explain which items were correct and which were missed. This conversation is clinically valuable for two reasons. First, the pattern of errors often provides diagnostic information that the overall score does not capture. Second, if you repeat the MoCA in the future, knowing your specific weakness domains allows you to target preparation more precisely.
Patients who actively engage with their assessment results and ask domain-level questions consistently report greater confidence in follow-up appointments and better adherence to any recommended cognitive health interventions. Knowledge of your own cognitive profile is a genuine clinical and personal asset.
Finally, remember that the MoCA is a starting point, not an endpoint. A normal score is genuinely reassuring, but it does not mean cognitive health should be taken for granted. Continuing to invest in sleep, exercise, diet, social engagement, and mental challenge is worthwhile regardless of any single assessment result.
A score suggesting mild cognitive impairment should prompt follow-up evaluation, not despair — many cases of apparent MCI are attributable to reversible causes, and even true MCI does not inevitably progress to dementia. The best outcome of any MoCA administration is an informed patient with a clearer picture of their cognitive health and a motivated partnership with their clinical team to support brain health over the long term.
MoCA Questions and Answers

MoCA Test Online: Complete Study Guide for the Montreal Cognitive Assessment

MoCA PDF: Download and Use the Montreal Cognitive Assessment Form

How to Pass the MoCA Exam in 2026 — Complete Study Guide

Montreal Cognitive Assessment Scoring: Complete Guide to MoCA Scores, Interpretation, and Preparation

MoCA Scoring and Interpretation: Complete Guide for Clinicians and Patients
About the Author

Educational Psychologist & Academic Test Preparation Expert
Columbia University Teachers CollegeDr. Lisa Patel holds a Doctorate in Education from Columbia University Teachers College and has spent 17 years researching standardized test design and academic assessment. She has developed preparation programs for SAT, ACT, GRE, LSAT, UCAT, and numerous professional licensing exams, helping students of all backgrounds achieve their target scores.
Join the Discussion
Connect with other students preparing for this exam. Share tips, ask questions, and get advice from people who have been there.
View discussion (7 replies)