Montreal Cognitive Assessment (MoCA): Scoring, Domains & Use 2026 August
⏳ What is the Montreal Cognitive Assessment? Learn MoCA domains, how scoring works, what scores mean, who administers it, and how to prepare for the

MoCA at a Glance
The Montreal Cognitive Assessment (MoCA) is a rapid screening tool used by healthcare professionals to detect mild cognitive impairment (MCI) and early-stage dementia. Developed by Dr. Ziad Nasreddine in 1996 and validated for widespread clinical use by 2005, the MoCA is now one of the most widely administered cognitive screening instruments in the world — used in primary care, neurology clinics, memory assessment centers, geriatric medicine, psychiatry, and research settings across more than 100 countries.
The MoCA is a 30-point assessment that takes approximately 10 minutes to administer and score. It covers seven cognitive domains: visuospatial and executive functioning, naming, memory, attention and concentration, language, abstraction, and orientation. Each domain contributes a fixed number of points to the total score. A score of 26 or above is generally considered normal; scores below 26 warrant further evaluation, though the clinical interpretation depends on the patient's history, education level, and the clinical context in which the assessment was administered.
The MoCA is not a diagnostic tool — it's a screening instrument. A low MoCA score indicates that cognitive difficulties may be present and that more comprehensive neuropsychological testing is warranted. It cannot diagnose Alzheimer's disease, vascular dementia, Lewy body dementia, or other specific conditions. What it does do — very effectively — is identify patients who warrant further evaluation, which is why it's become such a standard part of geriatric and memory clinic workflows.
The montreal cognitive assessment has significant advantages over the Mini-Mental State Examination (MMSE), the older cognitive screening tool it largely replaced in many clinical settings. The MoCA is more sensitive to mild cognitive impairment — the MMSE frequently misses early-stage cognitive changes that the MoCA detects — and it covers a broader range of cognitive domains. The MoCA was specifically designed to identify the subtle cognitive changes that mark the transition from normal aging to MCI, which is the population most clinically important to identify early.
This article covers every domain of the MoCA, how scoring works, what different score ranges indicate, who administers it, the training and certification requirements for clinicians, and preparation resources for healthcare professionals learning to administer and interpret the assessment.
Beyond its clinical uses, the MoCA has gained public attention in contexts where cognitive fitness is professionally relevant — notably in the evaluation of older adults applying for driving licenses, professional pilots undergoing fitness assessments, and public figures whose cognitive status has been publicly questioned. This broader context has made the MoCA more well-known to the general public than most cognitive screening tools, though its primary role remains clinical screening in healthcare settings.
The MoCA's development came from a recognized clinical problem: the Mini-Mental State Examination (MMSE), which dominated cognitive screening for decades, was not sensitive enough to detect the early cognitive changes that precede diagnosed dementia by years. Patients with clear functional decline and early biomarkers of Alzheimer's pathology were scoring in the normal MMSE range and being reassured inappropriately.
Dr. Nasreddine designed the MoCA specifically to be a more demanding test that would detect these subtler changes — and the validation studies confirmed it achieved that goal, with sensitivity for MCI of approximately 90% compared to the MMSE's 18% in some studies.
The MoCA isn't simply a questionnaire you hand to a patient. Proper administration requires specific instruction sequences, standardized timing for certain tasks, and consistent scoring criteria. MoCA Basic training certification is available through the official MoCA Cognition website — clinicians who administer the MoCA should complete this training to ensure reliable, valid results. Uncertified administration introduces scoring errors that undermine the tool's clinical value.
The MoCA's seven cognitive domains each assess distinct aspects of brain function. Understanding what each domain tests helps clinicians interpret score patterns — a patient who loses points specifically on delayed recall but performs normally on all other domains has a different clinical picture than one who loses points across executive functioning, attention, and language.
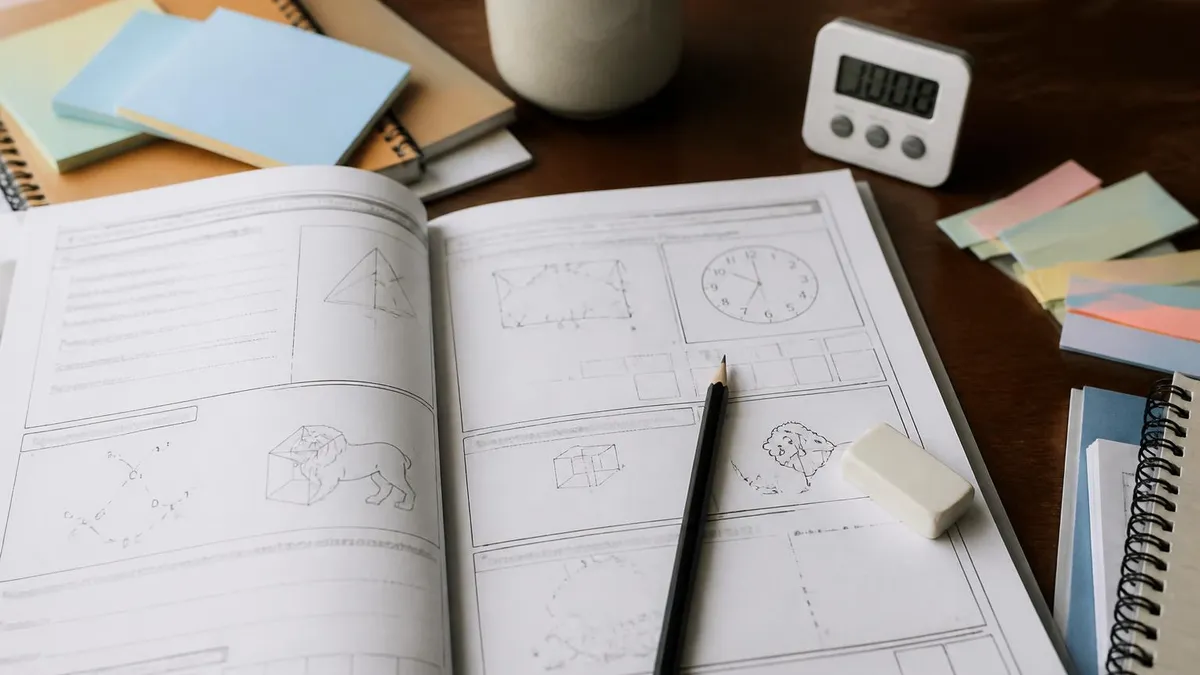
Visuospatial and Executive Functioning (5 points) is assessed through three tasks: an alternating trail-making task (connecting numbers and letters alternately), a cube copying task (drawing a three-dimensional cube), and a clock drawing task (drawing a clock face set to a specific time). These tasks assess spatial reasoning, planning, and the ability to execute a sequence of actions — all functions mediated by frontal and parietal brain regions that decline early in many forms of dementia.
Naming (3 points) asks patients to identify three pictures of animals (typically a lion, rhinoceros, and camel). This assesses language comprehension, word-finding, and semantic memory — functions involving temporal lobe structures that are often affected in Alzheimer's disease.
Memory and Delayed Recall (5 points) involves reading a list of five words, which the patient attempts to repeat twice. The words are tested again after other tasks have been completed — the delayed recall component specifically assesses hippocampal-dependent memory consolidation, which is among the earliest and most diagnostically significant domains affected in Alzheimer's disease pathology.
Attention and Concentration (6 points) covers four tasks: forward digit span (repeat a sequence of digits forward), backward digit span (repeat a sequence backward), a vigilance task (tap when you hear a specific letter in a random letter sequence), and serial 7 subtraction (subtract 7 from 100 repeatedly). These tasks assess working memory, sustained attention, and processing speed — domains mediated by frontal-subcortical circuits that are affected in both vascular cognitive impairment and Alzheimer's disease.
The MoCA test preparation resources at PracticeTestGeeks include practice questions across each cognitive domain, helping clinicians and students who are learning to administer and interpret the assessment become familiar with scoring criteria and the range of responses each task produces.
A common clinical question is how to interpret a MoCA score in a patient who completes the assessment slowly or who requires multiple repetitions of instructions. Standardized administration doesn't allow for extended time beyond what the protocol specifies — but clinical observation during the assessment is itself informative.
A patient who scores 28/30 but takes twice the expected time, shows significant frustration on the trail-making task, or requires instruction repetition multiple times may warrant closer follow-up than a patient who achieves the same score quickly and confidently. The score is one data point; the qualitative observations during administration add meaningful clinical depth.
MoCA Scoring Domains Explained
Language (3 points) tests repetition of two complex sentences and verbal fluency (name as many words beginning with a specific letter as possible in one minute). Sentence repetition assesses phonological working memory and language processing; verbal fluency assesses word retrieval and language access speed — both affected in frontotemporal dementia and early Alzheimer's. Abstraction (2 points) asks patients to identify the conceptual similarity between pairs of objects (how are a train and a bicycle similar?), assessing abstract reasoning mediated by frontal lobe function.
The MoCA is administered by trained healthcare professionals — physicians, nurses, nurse practitioners, physician assistants, neuropsychology technicians, occupational therapists, speech-language pathologists, and social workers — in any setting where cognitive screening is clinically indicated. Training in correct administration is available through MoCA Basic certification, a standardized online training course that covers how to administer and score each section of the assessment consistently and reliably.
Consistent, standardized administration is critical because small deviations in how tasks are presented can invalidate the results. For example, the word list in the memory section must be read at a specific pace; the timing of the letter vigilance task must be consistent; the instructions for clock drawing must be delivered verbatim. Clinicians who administer the MoCA from memory without maintaining the standardized script introduce error that makes their scores less reliable and harder to interpret in a longitudinal context — tracking a patient's score over time to detect progression requires that each administration uses identical procedures.
The moca pdf version of the assessment form and the administration guide are freely available through the official MoCA website for clinicians who have completed MoCA Basic certification. The certification is free, and Elsevier's MoCA basic training course is available online in multiple languages — the investment is modest for the clinical value it provides.
Serial MoCA administration — testing the same patient repeatedly over months or years — is the most clinically valuable use of the tool. A single MoCA score provides limited diagnostic information in isolation. But a pattern of declining scores over 18 months, even if each individual score still falls within the normal range, may be clinically significant. Documenting and tracking changes in domain-specific scores (rather than just total scores) provides even more granular information — a pattern of progressive delayed recall loss with preserved orientation may indicate a different underlying pathology than diffuse domain deterioration.
The moca adapter study preparation resources and the the moca los angeles exam preparation guide at PracticeTestGeeks support healthcare professionals who want to develop thorough familiarity with the MoCA's domains, scoring, and clinical interpretation before using it in practice settings.
In educational and training contexts, MoCA certification training helps clinicians not only learn correct administration procedure but also develop calibration on scoring — specifically, understanding the borderline cases where scoring decisions require clinical judgment. For example, when does a clock drawing score 2 vs. 1? When does an attempted word recall receive partial credit? The official training materials provide guidance and worked examples, but clinical exposure to a range of patient responses builds the intuitive scoring judgment that makes the MoCA a reliable and consistent tool across different administrators within a practice setting.
Before You Administer the MoCA
- Use the official MoCA form — versions with the five standard memory words only (avoid unofficial adaptations)
- Ensure the testing environment is quiet with minimal distractions
- Confirm the patient's hearing and vision are adequate for the tasks
- Have a pencil available for the drawing tasks (clock and cube)
- Note the patient's language and education level before scoring
- Allow the patient adequate time for tasks unless timing is specifically protocol-specified
- Record domain-specific scores, not just the total — pattern analysis provides more clinical information
- Never administer the MoCA as a standalone diagnostic — always integrate results with clinical history and judgment
The MoCA has known limitations: it's less sensitive in highly educated patients (ceiling effect), it may over-identify impairment in patients with low education levels even with the +1 adjustment, it's affected by hearing and visual impairments, and it's been validated primarily in English and may have lower validity in some cultural and linguistic contexts. Always interpret MoCA scores within the full clinical context — don't make clinical decisions based on a single score in isolation.
MoCA vs. MMSE: Clinical Comparison
- +MoCA: significantly more sensitive to mild cognitive impairment than MMSE
- +MoCA: broader domain coverage (7 domains vs. 5 for MMSE)
- +MoCA: specifically designed to detect MCI — the MMSE frequently misses early-stage decline
- +MoCA: better discrimination between normal aging and early pathological decline
- +MMSE: more widely known and historically accepted; decades of normative data
- +MMSE: shorter administration time (5–7 minutes vs. ~10 for MoCA)
- −MoCA: ceiling effect in highly educated patients can mask early decline
- −MoCA: requires certified administration training; not as simple to administer as MMSE
- −MoCA: copyright restrictions on forms limit free reproduction (unlike MMSE's public domain status)
- −MMSE: lower sensitivity for mild impairment — misses patients who need further evaluation
- −MMSE: doesn't assess executive function as thoroughly as MoCA
- −MMSE: may normalize scores for patients with early Alzheimer's who show significant clinical change
Preparing for the MoCA as a patient differs fundamentally from preparing for a professional exam. The MoCA is designed to assess your actual current cognitive function — not what you can memorize for the test. Clinicians are aware that patients who "study" for the MoCA by memorizing the word list or practicing clock drawing may produce scores that don't reflect their real cognitive status, which defeats the assessment's clinical purpose. Authentic MoCA results are far more useful to the clinical team responsible for your care than rehearsed performance.
That said, understanding what the MoCA tests — and what normal aging looks like versus clinical impairment — is legitimate and valuable for patients, families, and caregivers. Knowing that difficulty with delayed recall (forgetting the five words after a delay) is more diagnostically significant than difficulty with serial 7s (which many people find challenging regardless of cognitive status) helps patients and families contextualize results appropriately. Understanding the MoCA's structure helps families participate in clinical conversations about what the results mean for their loved one's care.
For healthcare professionals learning to administer the MoCA — medical students, nursing students, PA students, occupational therapy students, and clinicians cross-training in geriatric assessment — familiarity with the scoring criteria and the range of responses each domain elicits is genuinely important. Practice questions that cover MoCA scoring decisions, interpretation of domain-specific score patterns, and the clinical contexts in which the MoCA is and isn't appropriate build the clinical judgment that separates a skilled administrator from someone who can mechanically deliver the assessment without truly understanding what the results mean.
The comprehensive resources at PracticeTestGeeks — including domain-specific practice questions covering executive functioning, language, memory, attention, and all other MoCA domains — support clinicians and students who want to develop genuine command of the Montreal Cognitive Assessment as a clinical instrument. Mastering the MoCA isn't just about passing a certification module; it's about being able to use the tool with the clinical confidence and interpretive skill that makes cognitive screening genuinely useful for your patients.
The neuropsychological research literature on the MoCA continues to develop rapidly. Studies have now validated the tool across different cultural, linguistic, and demographic contexts; developed alternative equivalent versions that can be used for repeat testing without practice effects; and explored its utility in specific populations including Parkinson's disease, multiple sclerosis, HIV-associated neurocognitive disorders, and post-COVID cognitive symptoms. Healthcare professionals who work regularly with any of these populations benefit from familiarity with the population-specific normative data that supplement the original MoCA validation studies.
The MoCA works best as one component of a broader cognitive evaluation — alongside a clinical interview, functional assessment (how is the patient managing daily activities?), collateral history from family members or caregivers, and review of medications that may affect cognition. A patient who scores 24/30 on the MoCA but is managing all daily activities independently and shows no change from a baseline score taken two years earlier has a very different clinical picture than one with the same score whose family reports significant recent functional decline.
The Montreal Cognitive Assessment's reach has extended well beyond its origins in clinical dementia screening. Researchers use it as an outcome measure in clinical trials of medications and interventions targeting cognitive impairment. Sports medicine clinicians use it as part of concussion and head injury assessment protocols. Neurological rehabilitation programs use it to track cognitive recovery after stroke, traumatic brain injury, or surgery. Occupational medicine specialists use it in fitness-for-duty evaluations in safety-sensitive occupations.
In each of these contexts, the same principles of standardized administration and careful score interpretation apply — but the clinical questions being answered are different. A MoCA administered to a 70-year-old presenting with memory complaints in a primary care setting is answering the question "Does this patient need further neuropsychological evaluation?" A MoCA administered to a 45-year-old returning to work after a motor vehicle accident is answering the question "Has this patient's executive function and attention recovered sufficiently for them to safely perform their job duties?" The tool is the same; the clinical interpretation requires different reference points.
Understanding the full scope of the MoCA's applications — not just its use in geriatric memory clinics — helps healthcare professionals recognize when it's appropriate to use, when it isn't the right tool, and how to communicate results to patients and families in a way that's accurate, clinically useful, and compassionate.
The value of the MoCA extends across the entire arc of cognitive aging and neurological care. From the primary care physician screening a 68-year-old with a family history of Alzheimer's, to the occupational therapist assessing a stroke patient's readiness for discharge, to the researcher tracking cognitive outcomes in a clinical trial — the MoCA provides a common measurement language that supports clinical communication across specialties and settings.
Healthcare professionals who invest in understanding the MoCA deeply — not just as an administrative procedure but as a clinical tool with interpretive nuance — bring more value to their patients and their clinical teams. The assessment is brief, but the knowledge required to use it well is genuinely substantive.
The MoCA is used worldwide because it works — and because the clinicians who invest in learning it well return consistently better results, for their patients and for the healthcare teams who depend on their assessments.
MoCA Domains: Points and Clinical Significance
Declines early in frontotemporal dementia and Parkinson's-related cognitive impairment. The clock drawing task is sensitive to executive function deficits that patients and families may not report.
- :
- :
- :
- :
The most diagnostically significant domain for Alzheimer's disease detection. Impaired delayed recall with intact registration strongly suggests hippocampal pathology.
- :
- :
- :
- :
Attention deficits appear early in vascular cognitive impairment and delirium. Serial 7 subtraction is hard for many patients — the scoring gives credit for each correct subtraction even if the running total drifts.
- :
- :
- :
- :
Orientation loss in a patient who initially presents with only mild memory complaints is a red flag — it suggests the cognitive impairment is more advanced than the chief complaint implies.
- :
- :
- :
- :
MoCA Questions and Answers
About the Author

Educational Psychologist & Academic Test Preparation Expert
Columbia University Teachers CollegeDr. Lisa Patel holds a Doctorate in Education from Columbia University Teachers College and has spent 17 years researching standardized test design and academic assessment. She has developed preparation programs for SAT, ACT, GRE, LSAT, UCAT, and numerous professional licensing exams, helping students of all backgrounds achieve their target scores.
Join the Discussion
Connect with other students preparing for this exam. Share tips, ask questions, and get advice from people who have been there.
View discussion (7 replies)