WAIS-IV Manual: The Complete Training Guide for Clinicians and Students
Master the manual WAIS IV with our complete training guide. Administration rules, scoring, index scales & practice tests. 🎯 Start preparing today.
The manual WAIS IV — formally known as the Wechsler Adult Intelligence Scale, Fourth Edition Administration and Scoring Manual — is the authoritative reference document that governs how every licensed psychologist and trained clinician administers, scores, and interprets the most widely used adult intelligence test in the world. Understanding this manual is not optional for practitioners; it is the foundation upon which valid assessment rests. Whether you are a graduate student preparing for your first supervised administration or a seasoned clinician reviewing updated norms, mastering the wais iv manual is essential to delivering ethical, accurate, and legally defensible evaluations.
The wais was originally developed by David Wechsler in 1955 and has been revised four times since. The fourth edition, released in 2008 by Pearson Assessment, introduced significant structural changes including the reorganization of subtests into four Index Scales and the elimination of the traditional Verbal IQ and Performance IQ composite scores. These changes were grounded in contemporary factor-analytic research and reflect a more nuanced understanding of cognitive architecture. The manual codified these revisions in precise, standardized language so that every clinician follows an identical protocol regardless of geography or setting.
Clinicians who intend to administer the wais iq test must demonstrate competency not just in item delivery but in understanding the psychometric principles that underpin each subtest. The manual covers topics ranging from basal and ceiling rules to discontinuation criteria, reverse sequence administration, and the correct recording of verbatim responses. Each of these procedural details affects scoring accuracy, and even small deviations from standardized protocol can introduce construct-irrelevant variance that compromises the validity of an examinee's scores.
One dimension of training that many clinicians overlook is the correct sara wais — understanding how the name of the scale and its subtests are pronounced during rapport-building and client communication. While this may seem minor, professional communication with examinees, referral sources, and interdisciplinary teams requires comfort with the correct terminology. The manual itself dedicates space to ensuring practitioners can discuss the instrument fluently and accurately with all stakeholders involved in a psychological evaluation.
The manual also addresses the legal and ethical framework surrounding the wais test. Because intelligence testing has historically been misused as a basis for discrimination, the WAIS-IV manual contains explicit guidance on appropriate use cases, the qualifications required to purchase and administer the instrument, and the necessity of obtaining informed consent. Misuse of the instrument — including administration by unqualified individuals or use of outdated normative data — constitutes a violation of professional ethics codes enforced by the American Psychological Association and state licensing boards across the United States.
For examinees, understanding what the evaluation entails can reduce test anxiety and improve performance validity. Clinicians trained in the WAIS-IV manual learn how to provide standardized instructions that are both reassuring and non-leading. The manual's scripted introductory language is carefully worded to orient the examinee without cuing them to specific response strategies, preserving the integrity of the standardized assessment conditions under which the normative data were collected.
This article provides a comprehensive, structured tour of the WAIS-IV manual for clinicians in training, supervisors establishing training programs, and advanced students preparing for practicum and internship. We cover the manual's organization, administration requirements, scoring principles, index scale interpretation, and practical preparation strategies — everything you need to build genuine competency with this critical clinical instrument.
WAIS-IV by the Numbers
WAIS-IV Manual: How It Is Organized
The primary reference document detailing subtest-by-subtest administration instructions, discontinuation rules, basal and ceiling rules, timing requirements, and verbatim scoring criteria. This is the volume clinicians consult during and after every evaluation session.
Covers the psychometric foundations of the WAIS-IV including reliability coefficients, validity studies, factor structure, intercorrelation matrices, and guidance on clinical and special-group interpretation. Essential for understanding score meaning and test limitations.
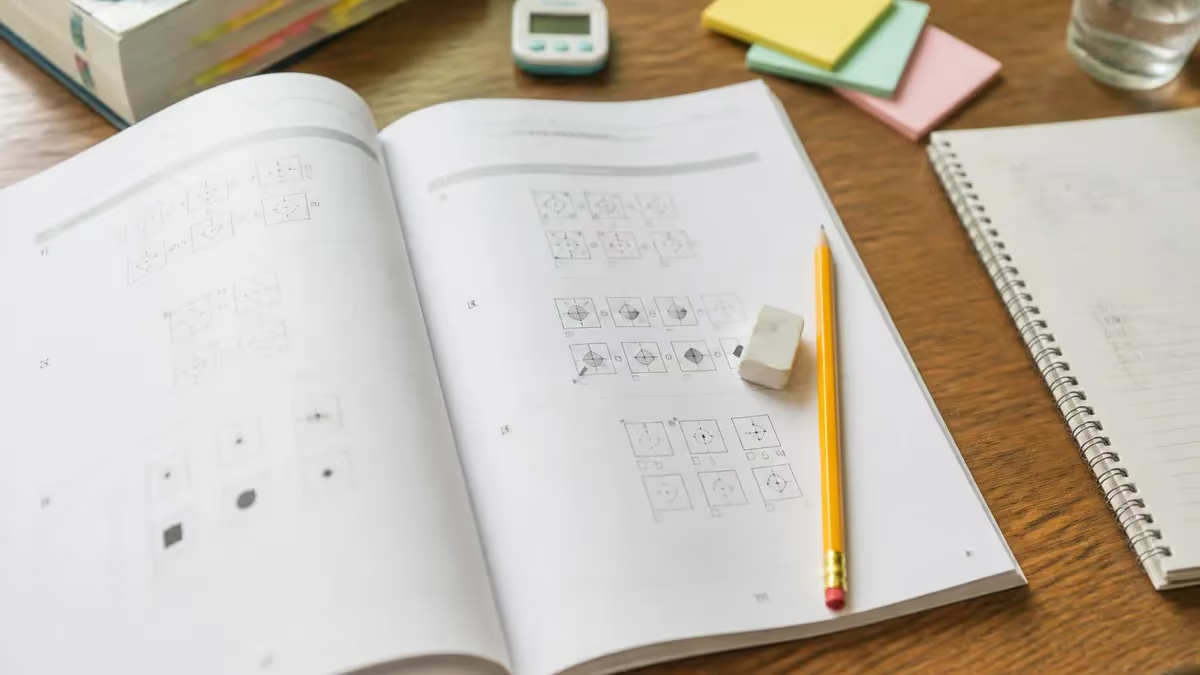
Physical test materials used during administration. Stimulus Books 1 and 2 contain visual items for subtests such as Block Design, Matrix Reasoning, and Visual Puzzles. Response booklets are used for written tasks including Coding and Symbol Search.
Standardized forms for recording verbatim responses, tallying raw scores, and converting to scaled scores and composite scores via lookup tables. The scoring key overlays allow rapid and accurate comparison of examinee responses against normative criteria.
Extensive appendices providing age-corrected scaled score conversions, composite score conversions, score difference significance tables, and base rate data for discrepancy analysis. These tables are used for virtually every clinical interpretation decision.
The wais-iv is a restricted instrument, meaning it may only be purchased and administered by professionals who meet specific qualification criteria established by Pearson Assessment. In the United States, this typically requires a doctoral-level degree in psychology, neuropsychology, or a closely related field, along with current licensure or certification in a state that authorizes psychological testing. Some jurisdictions also permit licensed educational psychologists and certain credentialed school psychologists to administer the instrument within the limits of their scope of practice.
Graduate students who are training to become psychologists can administer the WAIS-IV under the direct supervision of a licensed professional. The manual specifies that supervision must be competency-based rather than simply hour-based, meaning the supervising clinician must be satisfied that the trainee can administer all subtests accurately, maintain standardized conditions, record responses verbatim, calculate raw scores without error, and apply basal and ceiling rules consistently before independent administration is permitted. Most APA-accredited clinical and counseling psychology programs include formal WAIS-IV training as a required component of assessment coursework.
Understanding the wais 4 subtest requirements is critical for clinicians who plan to practice in neuropsychological or forensic settings. In these contexts, the stakes attached to cognitive assessment outcomes are particularly high — scores may influence competency determinations, disability claims, educational placement decisions, and legal proceedings. The manual explicitly states that practitioners working in high-stakes settings must be especially vigilant about maintaining standardized conditions, documenting any deviations from protocol, and appropriately qualifying their interpretations when non-standard conditions occurred.
Training programs typically follow a sequence that begins with observation of expert administration, proceeds to role-played practice with peers, and culminates in supervised live administrations with actual clients. The WAIS-IV manual recommends that trainees conduct at least five to ten complete administrations under supervision before attempting independent clinical use. During the observational phase, trainees are encouraged to follow along in the Administration and Scoring Manual simultaneously, noting the exact language used by the examiner and the timing procedures applied to timed subtests.
Continuing education is another dimension of WAIS-IV competency that the manual implicitly endorses. Psychometric research is ongoing, and since the fourth edition was published in 2008, numerous peer-reviewed studies have examined the instrument's performance across special clinical populations including traumatic brain injury, autism spectrum disorder, intellectual disability, learning disabilities, and late-life cognitive decline. Competent practitioners stay current with this literature and integrate emerging findings into their interpretive frameworks, even when those findings complicate straightforward application of the manual's interpretive guidelines.
The manual also provides guidance on testing accommodations for individuals with sensory, motor, or linguistic limitations. When a standard administration is not feasible — for example, when an examinee has significant upper-extremity motor impairment that precludes timed manual tasks — the manual outlines which subtests can be modified or omitted and how such modifications must be documented and disclosed in any written report. Importantly, the norms derived from the standardization sample do not apply when non-standard accommodations are used, and clinicians must exercise professional judgment in interpreting modified administrations.
For clinicians preparing to sit for specialty board certifications such as the American Board of Professional Psychology (ABPP) examination in clinical or neuropsychology, demonstrating mastery of the WAIS-IV manual is a core competency expectation. Oral examination panels routinely probe candidates on administration nuances, scoring edge cases, and the psychometric basis for interpretive claims. A thorough, direct engagement with the actual manual — not just secondary summaries — is therefore indispensable preparation for these high-stakes credentialing processes.
Understanding the WAIS-IV Index Scales and the Wechsler Adult Intelligence Scale (WAIS)
The Verbal Comprehension Index (VCI) measures crystallized intelligence — the knowledge and verbal reasoning abilities that an individual has accumulated over a lifetime of education and experience. Core subtests include Similarities, Vocabulary, and Information, with Comprehension serving as a supplemental subtest. High VCI scores are associated with strong verbal concept formation, lexical knowledge, and the ability to reason with abstract verbal material in a culturally embedded context.
Clinicians interpreting VCI scores must consider the examinee's educational history, language background, and exposure to English as a primary language. Individuals who were educated in non-English settings or who come from linguistically diverse households may score lower on VCI not due to reduced intellectual capacity but due to reduced exposure to the specific verbal content sampled by these subtests. The WAIS-IV manual advises practitioners to evaluate all composite scores in light of relevant background information and supplemental clinical data.
Strengths and Limitations of the WAIS-IV Manual as a Training Resource
- +Provides complete verbatim administration scripts, eliminating ambiguity in item delivery across clinicians
- +Includes detailed query and prompt guidance for ambiguous examinee responses on open-ended verbal subtests
- +Contains worked scoring examples for Similarities, Vocabulary, and Comprehension with multiple response quality levels
- +Offers comprehensive normative tables stratified by age group across the full 16–90 year range
- +Documents the psychometric rationale for every procedural rule, allowing clinicians to understand why standardization matters
- +Provides clinical and special-group studies data to support differential interpretation in neuropsychological contexts
- −Published in 2008, meaning normative data are now nearly two decades old and may not reflect contemporary population cognitive profiles
- −Does not include digital administration guidance, requiring separate supplemental resources for tablet-based administration
- −Scoring examples for some verbal subtests remain ambiguous at borderline response quality levels, requiring supervisor consultation
- −Limited guidance on culturally and linguistically diverse populations beyond brief acknowledgment of limitations
- −Physical manual is expensive to purchase and is not available in open-access digital format for trainees on limited budgets
- −Does not address the WAIS-5, leaving practitioners who transition to the updated edition without a direct comparison resource
WAIS-IV Administration Rules: Complete Preparation Checklist
- ✓Review the complete Administration and Scoring Manual from cover to cover before your first live administration attempt
- ✓Memorize the discontinuation rules for each subtest — errors required to stop vary across subtests and must not be confused
- ✓Practice delivering all verbatim instructions aloud until the scripted language feels natural and does not require constant manual reference
- ✓Time yourself on all timed subtests using a stopwatch during practice runs to ensure accurate bonus-point and time-limit application
- ✓Practice querying ambiguous verbal responses using the Q notation and the specific query language provided in the manual
- ✓Study the worked scoring examples for Similarities, Vocabulary, Comprehension, and Information to calibrate your 0-1-2 point judgments
- ✓Learn the correct reverse-sequence administration procedure for Digit Span and Arithmetic for examinees who struggle on early items
- ✓Prepare your testing room with all required materials organized in the prescribed order before the examinee arrives
- ✓Document any behavioral observations that may affect score interpretation, including fatigue, off-task behavior, and response latency
- ✓Calculate composite scores using the correct age band in the normative tables and double-check all arithmetic before finalizing the record form
The Most Common Administration Error Involves Discontinuation Rules
Research on WAIS-IV training errors consistently finds that clinicians-in-training most frequently err on discontinuation rules — either stopping too early and missing ceiling-level responses, or continuing too long and fatiguing the examinee unnecessarily. Memorizing the exact consecutive-failures criterion for each subtest, rather than assuming a uniform rule applies across all subtests, is the single highest-leverage study task for any trainee preparing for supervised administration.
Scoring the WAIS-IV accurately requires the clinician to work at two distinct levels simultaneously: the micro-level of individual item scoring and the macro-level of composite score computation. At the item level, subtests that involve open-ended verbal responses — particularly Similarities, Vocabulary, Comprehension, and Information — require the examiner to compare verbatim recorded responses against sample responses in the manual and assign scores of 0, 1, or 2 based on the conceptual sophistication demonstrated. This requires extensive familiarity with the manual's scoring criteria and, for borderline responses, judgment calibrated through supervised practice and consultation.
Many trainees underestimate the difficulty of verbal subtest scoring. A response to a Similarities item such as pairing two conceptually related objects may be objectively correct at a concrete level but incorrect at the abstract level required for full credit. The manual provides representative sample responses at each score level, but it cannot enumerate every possible response a clinician will encounter in clinical practice.
This is why the scoring of verbal subtests is considered a professional skill that develops over time and through ongoing consultation with more experienced practitioners rather than a mechanical process that can be mastered from the manual alone.
Processing speed subtests — Coding and Symbol Search — are scored more mechanically but introduce their own sources of error. Coding requires the examiner to accurately count completed symbols within the 120-second time limit, using the scoring key template provided. Common errors include miscounting symbols, failing to penalize for incorrectly completed items, or allowing extra time beyond the specified limit. Symbol Search scoring requires distinguishing target symbols correctly matched by the examinee from incorrect responses, using a similar template overlay. Both subtests demand that the examiner maintain undivided attention during the administration to avoid timing errors.
Raw scores are converted to scaled scores using the age-corrected normative tables in Appendix A of the Administration and Scoring Manual. Crucially, the examiner must identify the correct age band for the examinee and use only the table corresponding to that band. Using the wrong age table is a serious scoring error that will yield systematically biased composite scores.
Each raw score is converted to a scaled score with a mean of 10 and a standard deviation of 3. These scaled scores are then summed within each Index Scale and converted to composite scores with a mean of 100 and a standard deviation of 15 using a second set of conversion tables.
The Full Scale IQ (FSIQ) is derived from the sum of scaled scores across the 10 core subtests and represents the most comprehensive single summary of an examinee's cognitive functioning. However, the manual is explicit that the FSIQ should not be interpreted as a unitary, fixed trait, but as one summary statistic within a profile of abilities that may show meaningful variation across Index Scales.
When the FSIQ is based on markedly discrepant Index scores, its interpretation as a summary of overall ability becomes questionable, and the manual recommends considering alternative composite scores such as the General Ability Index (GAI) or the Cognitive Proficiency Index (CPI).
Score difference analysis is a critical component of WAIS-IV interpretation addressed extensively in the Technical and Interpretive Manual. Clinicians determine whether differences between Index scores — for example, a gap between Verbal Comprehension and Processing Speed — are statistically significant and whether they are abnormally rare in the normative population.
The manual provides critical values for significance at both the .05 and .15 probability levels, and base rate tables showing what percentage of the normative sample obtained a given size of discrepancy. Understanding the distinction between statistical significance and clinical unusualness is one of the more conceptually demanding aspects of WAIS-IV interpretation.
The wais iq score — technically the Full Scale IQ — is frequently misunderstood by lay audiences who equate it with an immutable, biologically determined capacity. Clinicians trained in the WAIS-IV manual understand that the FSIQ reflects the interaction between underlying neurological capacity and the accumulated impact of educational opportunity, socioeconomic resources, linguistic exposure, and testing conditions on the day of administration. A comprehensive written report contextualizes the FSIQ within this broader understanding, and the manual encourages this interpretive sophistication as an ethical obligation of every practitioner who uses the instrument.
The WAIS-5 was released by Pearson Assessment in 2024 with updated norms, revised subtests, and a restructured composite score framework. The WAIS-IV Administration and Scoring Manual does NOT apply to WAIS-5 administration — using WAIS-IV procedures with WAIS-5 materials, or vice versa, constitutes a serious standardization violation that invalidates the assessment. Verify which edition your training program uses and purchase or access only the corresponding manual and normative materials.
Preparing for a career that regularly involves WAIS administration means developing a long-term relationship with both the instrument and its evolving research base. Many clinical neuropsychologists administer the WAIS or its revision hundreds of times over the course of a career, and expert-level performance emerges from that accumulated experience alongside deliberate efforts to stay current with the literature. The manual serves as the anchor of this practice, but it is the practitioner's ongoing engagement with supervision, peer consultation, and continuing education that transforms manual knowledge into genuine clinical expertise.
One practical preparation strategy for trainees is to create a personal quick-reference card summarizing the discontinuation criteria, timing limits, and reverse-sequence rules for every subtest. While this card should never replace the manual during actual administration, creating it forces active recall of the most procedurally critical information and reveals gaps in knowledge before they manifest as errors in a live evaluation. Supervisors often recommend that trainees construct these cards from memory and then check them against the actual manual — a self-testing strategy that dramatically improves retention of procedural details.
Role-playing administrations with peers is another evidence-based preparation strategy widely used in clinical training programs. When a peer plays the role of the examinee and deliberately gives ambiguous or scorable-at-multiple-levels verbal responses, the trainee-administrator must make real-time scoring and querying decisions under the gentle pressure of performance. This simulation mirrors the cognitive load of actual clinical administration more effectively than solo study and reveals procedural automaticity gaps that reading alone cannot expose.
Video recording practice administrations — with appropriate consent in training contexts — allows trainees to review their own performance and identify specific procedural deviations that might otherwise go unnoticed in the moment. Supervisors who review recorded administrations alongside the trainee can provide targeted, behavior-specific feedback rather than general encouragement. Research on motor skill learning, which closely parallels the procedural skill demands of psychological assessment, consistently shows that specific corrective feedback produces faster skill acquisition than generic positive reinforcement.
The transition from student to professional includes staying informed about updates and developments in the broader WAIS ecosystem. The release of the wais 5 in 2024 represents the most recent major revision, featuring co-normed updates and new composite score structures that differ meaningfully from the WAIS-IV framework. Clinicians who trained exclusively on the fourth edition will need to actively invest in re-training when their clinical settings transition to the new edition, and supervisors must ensure that training programs address both editions during any transitional period when both instruments may be in use concurrently.
Ethical competency requires that clinicians also understand the historical and sociopolitical context of intelligence testing in the United States. The WAIS-IV manual acknowledges the ongoing scientific debate about mean score differences across demographic groups and explicitly cautions against using group membership as a basis for score interpretation or adjustment outside the guidance provided by the normative data. Practitioners operating in forensic, educational, or disability-determination contexts face particular scrutiny on this dimension, and the manual's guidance must be read alongside the APA's published guidelines on test bias and fairness.
Finally, connecting daily study of the wais iq manual to broader theoretical frameworks in cognitive psychology and neuropsychology deepens the practitioner's interpretive sophistication. Understanding how Index Scale constructs relate to Cattell-Horn-Carroll (CHC) theory, working memory models, processing efficiency frameworks, and neural networks of executive control transforms the WAIS-IV from a scoring exercise into a window onto the structure of human cognition. The manual is the procedural backbone, but theory is what gives its numbers clinical life and meaning.
Building lasting proficiency with the WAIS-IV manual is an active, iterative process that extends well beyond a single semester of graduate training. Experienced supervisors consistently report that the biggest gap between novice and expert WAIS-IV administrators is not knowledge of rules but the ability to maintain standardized conditions while simultaneously monitoring examinee behavior, recording verbatim responses, managing timing, and calibrating the interpersonal rapport that keeps an examinee engaged across a 60-to-90-minute evaluation. Developing this multitasking capacity requires deliberate, repeated practice under supervision.
One often-overlooked aspect of WAIS-IV manual mastery is understanding the instrument's psychometric limitations as clearly as its strengths. The manual's Technical and Interpretive volume details test-retest reliability coefficients that vary across subtests — Processing Speed subtests show the greatest practice effects on retest, while verbal subtests demonstrate somewhat smaller gains. Clinicians who evaluate the same individual multiple times must factor these practice-effect estimates into their interpretations, using the manual's published retest data to distinguish genuine cognitive change from statistical artifact.
Group-based training workshops offered by Pearson, university continuing education programs, and professional organizations like the National Academy of Neuropsychology (NAN) provide structured opportunities to refine WAIS-IV skills beyond what individual supervision alone can offer. These workshops typically include live demonstration administrations, group scoring exercises with norm-referenced feedback, and case-based discussion of complex interpretive scenarios. Many clinicians find that attending a structured workshop after initial training consolidates their procedural skills and exposes gaps that were not apparent during solo practice.
For clinicians who work with older adults — a growing segment of the population given demographic trends — the WAIS-IV's extended age ceiling of 90 years is a particularly valuable feature. The normative sample for the oldest age bands (70–74, 75–79, 80–84, 85–90) was carefully designed to be representative of community-dwelling older adults rather than institutionalized populations, which is an important distinction for valid interpretation. Clinicians must nonetheless be alert to sensory and motor confounds that become increasingly prevalent in older examinees and document all observed limitations that may have influenced subtest performance.
Supervision documentation is a procedural requirement in most training programs and is strongly recommended in the WAIS-IV manual's professional use section. Supervisors should maintain records of each trainee's observed administrations, the specific procedural competencies evaluated, and any corrective feedback provided. This documentation protects both the supervisor and the trainee in the event of a professional complaint and provides a structured record of competency development that can be shared with future supervisors, internship training directors, or licensing boards.
Finally, developing comfort with communicating WAIS-IV results to diverse audiences is as important as the technical skill of administration and scoring. Examinees and their families deserve clear, jargon-free explanations of what scores mean in practical terms. Referral sources such as physicians, attorneys, educators, and rehabilitation specialists have their own professional frames of reference that shape how they understand and use cognitive assessment data.
The WAIS-IV manual does not explicitly address communication strategies, but the ethical codes underpinning it make clear that valid assessment is not complete until results are communicated accurately and accessibly to all parties who have a legitimate need to understand them.
Returning to the manual regularly — even after years of clinical experience — is a hallmark of expert WAIS-IV practitioners. Procedural drift, in which small deviations from standardized administration accumulate over time and become habits, is a documented phenomenon in assessment psychology. Periodic self-review of the manual, participation in peer consultation groups, and openness to feedback from supervisors and colleagues are the professional habits that sustain long-term assessment competency and protect the validity of every evaluation conducted throughout a clinical career.
WAIS Questions and Answers

WAIS Pronunciation, Meaning, and Everything You Need to Know About the Test

WAIS Block Design Test: What It Measures & How to Prep
Wechsler Adult Intelligence Scale (WAIS): What It Measures and How It Works

WAIS Version History: From WAIS-I to WAIS-5 — How the Test Has Evolved

WAIS-IV Digit Span: What It Measures, How It Works, and How to Prepare
About the Author

Licensed Psychologist & Mental Health Licensing Exam Expert
Northwestern UniversityDr. Nicole Warren holds a PhD in Clinical Psychology from Northwestern University and is licensed as both a Professional Counselor (LPC) and Clinical Social Worker (LCSW). She has 14 years of clinical practice in cognitive-behavioral therapy and trauma-informed care, and coaches psychology and counseling graduates through the EPPP, ASWB, NCE, and state mental health licensing examinations.